Evaluation of the Analgesic Efficacy of Bilateral Ultrasound-Guided Transversus Thoracic Muscle Plane Block on Post-Sternotomy Pain: A Randomized Controlled Trial.
{"title":"Evaluation of the Analgesic Efficacy of Bilateral Ultrasound-Guided Transversus Thoracic Muscle Plane Block on Post-Sternotomy Pain: A Randomized Controlled Trial.","authors":"Hoda Shokri, Ihab Ali, Amr A Kasem","doi":"10.2147/LRA.S338685","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>Transverse thoracic block is a new perioperative analgesic method for post-sternotomy discomfort. This study discusses the efficacy of an ultrasound-guided transversus thoracic muscle plane block (TTPB) in patients undergoing heart surgery, including sternotomy.</p><p><strong>Patients and methods: </strong>In this prospective trial, 60 patients were randomly assigned to two groups: transversus (T) or general anesthesia (GA). Patients in the T group received TTPB with GA and 15 mL of 0.25% bupivacaine was administered on either side. Patients in the GA group received TTPB along with GA, but 15 mL saline was injected on either side instead. The patients were followed up postoperatively. The percentage of patients receiving additional opioids, extubation time, intensive care unit (ICU) length, postoperative morphine dose, and adverse events were documented.</p><p><strong>Results: </strong>The percentage of patients requiring additional morphine was significantly lower in the T group (p<0.015). Pain scores were comparable between the groups at extubation time and 18 h postoperatively. At 8, 12, and 24 h after surgery, pain scores in the T group were significantly lower (P<0.001). The total amount of morphine required after surgery was much lower in the T group (8±0.74 mg), and the duration to initial analgesic necessity was significantly greater in the GA group (P<0.001). Patients in the GA group had a considerably longer ventilation time (11.07±0.64) (P<0.001). The ICU stay in the T group was substantially shorter (P<0.001), and postoperative complications were comparable.</p><p><strong>Conclusion: </strong>For patients undergoing heart surgery, TTPB offers sufficient postoperative pain control, resulting in lower pain scores, lower postoperative analgesic doses, shorter extubation times, and shorter ICU stay lengths.</p>","PeriodicalId":18203,"journal":{"name":"Local and Regional Anesthesia","volume":"14 ","pages":"145-152"},"PeriodicalIF":1.9000,"publicationDate":"2021-11-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/ec/21/lra-14-145.PMC8594901.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Local and Regional Anesthesia","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/LRA.S338685","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose: Transverse thoracic block is a new perioperative analgesic method for post-sternotomy discomfort. This study discusses the efficacy of an ultrasound-guided transversus thoracic muscle plane block (TTPB) in patients undergoing heart surgery, including sternotomy.
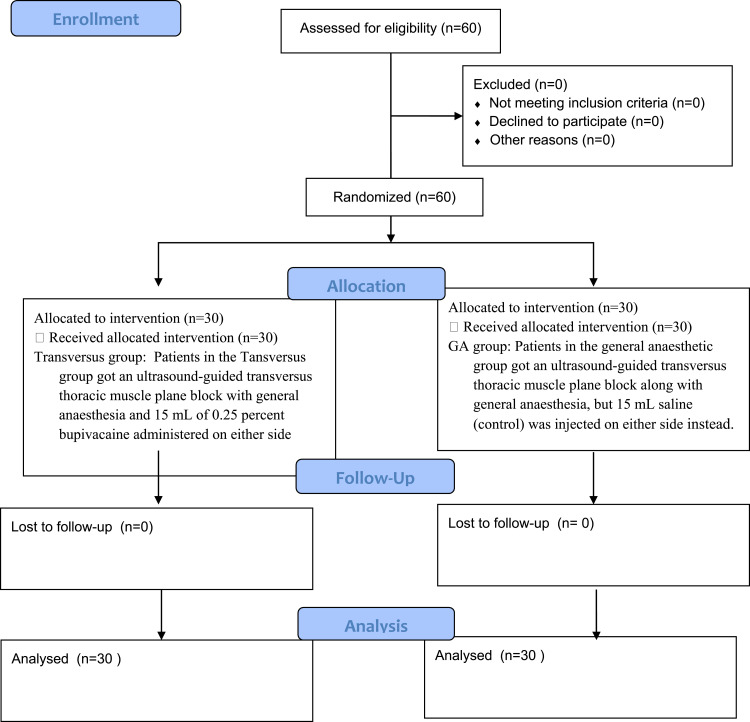
Patients and methods: In this prospective trial, 60 patients were randomly assigned to two groups: transversus (T) or general anesthesia (GA). Patients in the T group received TTPB with GA and 15 mL of 0.25% bupivacaine was administered on either side. Patients in the GA group received TTPB along with GA, but 15 mL saline was injected on either side instead. The patients were followed up postoperatively. The percentage of patients receiving additional opioids, extubation time, intensive care unit (ICU) length, postoperative morphine dose, and adverse events were documented.
Results: The percentage of patients requiring additional morphine was significantly lower in the T group (p<0.015). Pain scores were comparable between the groups at extubation time and 18 h postoperatively. At 8, 12, and 24 h after surgery, pain scores in the T group were significantly lower (P<0.001). The total amount of morphine required after surgery was much lower in the T group (8±0.74 mg), and the duration to initial analgesic necessity was significantly greater in the GA group (P<0.001). Patients in the GA group had a considerably longer ventilation time (11.07±0.64) (P<0.001). The ICU stay in the T group was substantially shorter (P<0.001), and postoperative complications were comparable.
Conclusion: For patients undergoing heart surgery, TTPB offers sufficient postoperative pain control, resulting in lower pain scores, lower postoperative analgesic doses, shorter extubation times, and shorter ICU stay lengths.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
