{"title":"Clinical profile and retinal nerve fibre layer thickness of optic disc oedema patients at a tertiary care institute in North India.","authors":"Gitanjli Sood, Ramanuj Samanta, Devesh Kumawat, Ajai Agrawal, Anupam Singh","doi":"10.1177/25158414211072634","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Optic disc oedema (ODE) is an important manifestation in various ocular as well as systemic disorders. Measurement of retinal nerve fibre layer (RNFL) thickness in ODE patients may help in monitoring the progress of the disease and treatment response.</p><p><strong>Objective: </strong>To assess the clinical characteristics, aetiology and retinal nerve fibre layer (RNFL) imaging features of optic disc oedema (ODE) patients.</p><p><strong>Design: </strong>A retrospective observational study.</p><p><strong>Methods: </strong>This hospital-based study included performed for patients presenting with unilateral or bilateral ODE at the ophthalmology outpatient department of a tertiary institute between January 2019 and December 2019. Clinical features of all ODE patients were noted. RNFL thickness was measured by spectral-domain optical coherence tomography (Cirrus 500, Carl Zeiss Meditec, Dublin, CA, USA).</p><p><strong>Results: </strong>Sixty-four patients with ODE were seen with female preponderance (56.2%). The mean age of presentation was 36.8 ± 13.8 years. Bilateral ODE was seen in 57.8% patients. The most common cause of bilateral ODE was idiopathic intracranial hypertension (IIH) and vascular papillopathy. Retinal vein occlusion (RVO)-associated ODE was the most common unilateral presentation. Presenting visual acuity was best with IIH and worst with anterior ischaemic optic neuropathy (AION). The mean duration of symptoms was maximum with intracranial space-occupying lesion associated papilloedema and minimum with AION. The mean RNFL thickness was highest in uveitis-associated ODE, followed by compressive ON, and IIH. A positive correlation was noted between clinical ODE severity and RNFL thickness. All aetiological categories (except uveitic and compressive) had maximum RNFL thickening in the inferior quadrant and minimum in the temporal quadrant.</p><p><strong>Conclusion: </strong>The current study provides a clinical profile and RNFL measurements of ODE patients at this locality. The clinical severity of ODE correlated positively with RNFL thickness and most of the categories of ODE followed the normative pattern of RNFL thickness (inferior > superior > nasal > temporal) despite thickening.</p>","PeriodicalId":23054,"journal":{"name":"Therapeutic Advances in Ophthalmology","volume":" ","pages":"25158414211072634"},"PeriodicalIF":2.3000,"publicationDate":"2022-02-14","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/f0/3e/10.1177_25158414211072634.PMC8854232.pdf","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Therapeutic Advances in Ophthalmology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/25158414211072634","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"OPHTHALMOLOGY","Score":null,"Total":0}
引用次数: 1
Abstract
Background: Optic disc oedema (ODE) is an important manifestation in various ocular as well as systemic disorders. Measurement of retinal nerve fibre layer (RNFL) thickness in ODE patients may help in monitoring the progress of the disease and treatment response.
Objective: To assess the clinical characteristics, aetiology and retinal nerve fibre layer (RNFL) imaging features of optic disc oedema (ODE) patients.
Design: A retrospective observational study.
Methods: This hospital-based study included performed for patients presenting with unilateral or bilateral ODE at the ophthalmology outpatient department of a tertiary institute between January 2019 and December 2019. Clinical features of all ODE patients were noted. RNFL thickness was measured by spectral-domain optical coherence tomography (Cirrus 500, Carl Zeiss Meditec, Dublin, CA, USA).
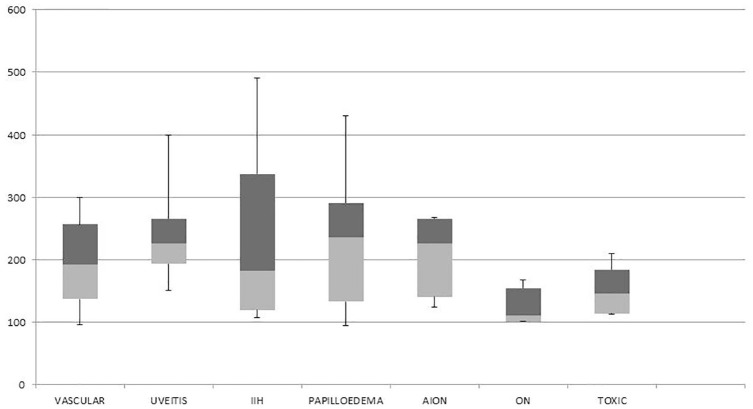
Results: Sixty-four patients with ODE were seen with female preponderance (56.2%). The mean age of presentation was 36.8 ± 13.8 years. Bilateral ODE was seen in 57.8% patients. The most common cause of bilateral ODE was idiopathic intracranial hypertension (IIH) and vascular papillopathy. Retinal vein occlusion (RVO)-associated ODE was the most common unilateral presentation. Presenting visual acuity was best with IIH and worst with anterior ischaemic optic neuropathy (AION). The mean duration of symptoms was maximum with intracranial space-occupying lesion associated papilloedema and minimum with AION. The mean RNFL thickness was highest in uveitis-associated ODE, followed by compressive ON, and IIH. A positive correlation was noted between clinical ODE severity and RNFL thickness. All aetiological categories (except uveitic and compressive) had maximum RNFL thickening in the inferior quadrant and minimum in the temporal quadrant.
Conclusion: The current study provides a clinical profile and RNFL measurements of ODE patients at this locality. The clinical severity of ODE correlated positively with RNFL thickness and most of the categories of ODE followed the normative pattern of RNFL thickness (inferior > superior > nasal > temporal) despite thickening.
背景:视盘水肿(ODE)是各种眼部及全身疾病的重要表现。测量ODE患者的视网膜神经纤维层(RNFL)厚度可能有助于监测疾病进展和治疗反应。目的:探讨视盘水肿(ODE)患者的临床特点、病因及视网膜神经纤维层(RNFL)影像学特征。设计:回顾性观察性研究。方法:这项以医院为基础的研究纳入了2019年1月至2019年12月在某大专院校眼科门诊就诊的单侧或双侧ODE患者。记录所有ODE患者的临床特征。采用光谱域光学相干断层扫描(Cirrus 500, Carl Zeiss Meditec, Dublin, CA, USA)测量RNFL厚度。结果:64例ODE患者中,女性居多(56.2%)。平均发病年龄36.8±13.8岁。57.8%的患者出现双侧ODE。双侧ODE最常见的原因是特发性颅内高压(IIH)和血管乳头病。视网膜静脉阻塞(RVO)相关的ODE是最常见的单侧表现。IIH患者表现视力最佳,前缺血性视神经病变(AION)最差。症状的平均持续时间在颅内占位性病变相关的乳头状水肿中最长,在AION中最短。uvetis相关性ODE的RNFL平均厚度最高,其次是压缩性ON和IIH。临床ODE严重程度与RNFL厚度呈正相关。所有病因分类(除了葡萄膜和压缩)下象限RNFL增厚最大,颞象限最小。结论:目前的研究提供了该地区ODE患者的临床概况和RNFL测量。ODE的临床严重程度与RNFL厚度呈正相关,尽管增厚,但大多数ODE的RNFL厚度均符合标准模式(下>上>鼻>颞)。





 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
