Hasan M Al Dorzi, Alaaeldien G Ghanem, Mohamed Moneer Hegazy, Amal AlMatrood, John Alchin, Mohammed Mutairi, Ahmad Aqeil, Yaseen M Arabi
{"title":"Humidification during mechanical ventilation to prevent endotracheal tube occlusion in critically ill patients: A case control study.","authors":"Hasan M Al Dorzi, Alaaeldien G Ghanem, Mohamed Moneer Hegazy, Amal AlMatrood, John Alchin, Mohammed Mutairi, Ahmad Aqeil, Yaseen M Arabi","doi":"10.4103/atm.atm_135_21","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Endotracheal tube (ETT) occlusion is a potentially life-threatening event. This study describes a quality improvement project to prevent ETT occlusion in critically ill patients.</p><p><strong>Methods: </strong>After a cluster of clinically significant ETT occlusion incidents at a tertiary-care intensive care unit (ICU), the root cause analysis suggested that the universal use of heat moisture exchangers (HMEs) was a major cause. Then, we prospectively audited new ETT occlusion incidents after changing our practices to evidence-based active and passive humidification during mechanical ventilation (MV). We also compared the outcomes of affected patients with matched controls.</p><p><strong>Results: </strong>During 100 weeks, 18 incidents of clinically significant ETT occlusion occurred on a median of 7 days after intubation (interquartile range, 4.8-9.5): 8 in the 10 weeks before and 10 in the 90 weeks after changing humidification practices (8.1 vs. 1.0 incidents per 1000 ventilator days, respectively). The incidents were not suspected in 94.4%, the peak airway pressure was >30 cm H<sub>2</sub>O in only 25%, and 55.6% were being treated for pneumonia when ETT occlusion occurred. Compared with 51 matched controls, ETT occlusion cases had significantly longer MV duration (median of 13.5 vs. 4.0 days; <i>P</i> = 0.002) and ICU stay (median of 26.5 vs. 11.0 days; <i>P</i> = 0.006) and more tracheostomy (55.6% vs. 9.8%; <i>P</i> < 0.001). The hospital mortality was similar in cases and controls.</p><p><strong>Conclusions: </strong>The rate of ETT occlusion decreased after changing humidification practices from universal HME use to evidence-based active and passive humidification. ETT occlusion was associated with more tracheostomy and a longer duration of MV and ICU stay.</p>","PeriodicalId":50760,"journal":{"name":"Annals of Thoracic Medicine","volume":"17 1","pages":"37-43"},"PeriodicalIF":2.3000,"publicationDate":"2022-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/48/1d/ATM-17-37.PMC8809127.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of Thoracic Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.4103/atm.atm_135_21","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/1/14 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Endotracheal tube (ETT) occlusion is a potentially life-threatening event. This study describes a quality improvement project to prevent ETT occlusion in critically ill patients.
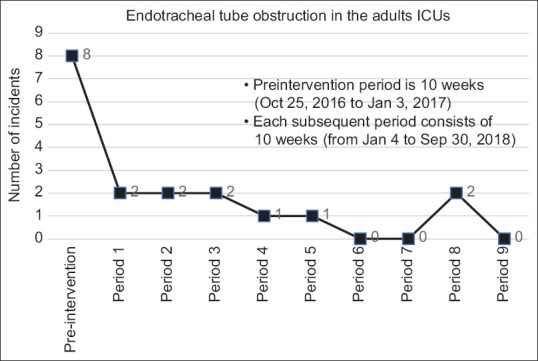
Methods: After a cluster of clinically significant ETT occlusion incidents at a tertiary-care intensive care unit (ICU), the root cause analysis suggested that the universal use of heat moisture exchangers (HMEs) was a major cause. Then, we prospectively audited new ETT occlusion incidents after changing our practices to evidence-based active and passive humidification during mechanical ventilation (MV). We also compared the outcomes of affected patients with matched controls.
Results: During 100 weeks, 18 incidents of clinically significant ETT occlusion occurred on a median of 7 days after intubation (interquartile range, 4.8-9.5): 8 in the 10 weeks before and 10 in the 90 weeks after changing humidification practices (8.1 vs. 1.0 incidents per 1000 ventilator days, respectively). The incidents were not suspected in 94.4%, the peak airway pressure was >30 cm H2O in only 25%, and 55.6% were being treated for pneumonia when ETT occlusion occurred. Compared with 51 matched controls, ETT occlusion cases had significantly longer MV duration (median of 13.5 vs. 4.0 days; P = 0.002) and ICU stay (median of 26.5 vs. 11.0 days; P = 0.006) and more tracheostomy (55.6% vs. 9.8%; P < 0.001). The hospital mortality was similar in cases and controls.
Conclusions: The rate of ETT occlusion decreased after changing humidification practices from universal HME use to evidence-based active and passive humidification. ETT occlusion was associated with more tracheostomy and a longer duration of MV and ICU stay.
期刊介绍:
The journal will cover studies related to multidisciplinary specialties of chest medicine, such as adult and pediatrics pulmonology, thoracic surgery, critical care medicine, respiratory care, transplantation, sleep medicine, related basic medical sciences, and more. The journal also features basic science, special reports, case reports, board review , and more. Editorials and communications to the editor that explore controversial issues and encourage further discussion by physicians dealing with chest medicine.





 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
