Sherby Suet-Ying Pang, Evan Fang, Kam Wai Chen, Matthew Leung, Velda Ling-Yu Chow, Christian Fang
{"title":"Patient-specific 3D-printed helmet for post-craniectomy defect - a case report.","authors":"Sherby Suet-Ying Pang, Evan Fang, Kam Wai Chen, Matthew Leung, Velda Ling-Yu Chow, Christian Fang","doi":"10.1186/s41205-022-00131-1","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Patients who undergo decompressive craniectomy (DC) are often fitted with a helmet that protects the craniectomy site from injury during rehabilitation. However, conventional \"one-size-fits-all\" helmets may not be feasible for certain craniectomy defects. We describe the production and use of a custom 3D-printed helmet for a DC patient where a conventional helmet was not feasible due to the craniectomy defect configuration.</p><p><strong>Case presentation: </strong>A 65-year-old male with ethmoid sinonasal carcinoma underwent cranionasal resection and DC with free vastus lateralis flap reconstruction to treat cerebrospinal fluid leakage. He required an external helmet to protect the craniectomy site, however, the rim of a conventional helmet compressed the craniectomy site, and the straps compressed the vascular pedicle of the muscle flap. Computed topography (CT) scans of the patient's cranium were imported into 3D modelling software and used to fabricate a patient-specific, strapless helmet using fused deposition modelling (FDM). The final helmet fit the patient perfectly and circumvented the compression issues, while also providing better cosmesis than the conventional helmet. Four months postoperatively, the helmet remains intact and in use.</p><p><strong>Conclusions: </strong>3D printing can be used to produce low-volume, patient-specific external devices for rehabilitation where standardized adjuncts are not optimal. Once initial start-up costs and training are overcome, these devices can be produced by surgeons themselves to meet a wide range of clinical needs.</p>","PeriodicalId":72036,"journal":{"name":"3D printing in medicine","volume":" ","pages":"4"},"PeriodicalIF":3.1000,"publicationDate":"2022-01-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8796519/pdf/","citationCount":"3","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"3D printing in medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s41205-022-00131-1","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING","Score":null,"Total":0}
引用次数: 3
Abstract
Background: Patients who undergo decompressive craniectomy (DC) are often fitted with a helmet that protects the craniectomy site from injury during rehabilitation. However, conventional "one-size-fits-all" helmets may not be feasible for certain craniectomy defects. We describe the production and use of a custom 3D-printed helmet for a DC patient where a conventional helmet was not feasible due to the craniectomy defect configuration.
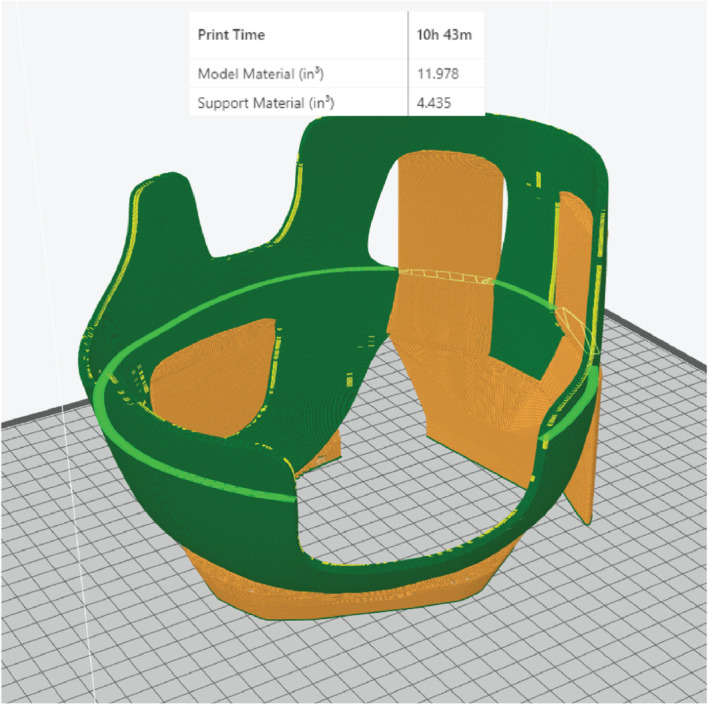
Case presentation: A 65-year-old male with ethmoid sinonasal carcinoma underwent cranionasal resection and DC with free vastus lateralis flap reconstruction to treat cerebrospinal fluid leakage. He required an external helmet to protect the craniectomy site, however, the rim of a conventional helmet compressed the craniectomy site, and the straps compressed the vascular pedicle of the muscle flap. Computed topography (CT) scans of the patient's cranium were imported into 3D modelling software and used to fabricate a patient-specific, strapless helmet using fused deposition modelling (FDM). The final helmet fit the patient perfectly and circumvented the compression issues, while also providing better cosmesis than the conventional helmet. Four months postoperatively, the helmet remains intact and in use.
Conclusions: 3D printing can be used to produce low-volume, patient-specific external devices for rehabilitation where standardized adjuncts are not optimal. Once initial start-up costs and training are overcome, these devices can be produced by surgeons themselves to meet a wide range of clinical needs.




 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
