Acute but not chronic heart failure is associated with higher mortality among patients hospitalized with pneumonia: An analysis of a nationwide database
Essa Hariri , Niti G. Patel , Elias Bassil , Milad Matta , Pei-Chun Yu , Quinn R. Pack , Michael B. Rothberg
{"title":"Acute but not chronic heart failure is associated with higher mortality among patients hospitalized with pneumonia: An analysis of a nationwide database","authors":"Essa Hariri , Niti G. Patel , Elias Bassil , Milad Matta , Pei-Chun Yu , Quinn R. Pack , Michael B. Rothberg","doi":"10.1016/j.ajmo.2022.100013","DOIUrl":null,"url":null,"abstract":"<div><h3>Background</h3><p>Among patients admitted for pneumonia, heart failure (HF) is associated with worse outcomes. It is unclear whether this association is due to acute HF exacerbations, complex medical management, or chronic co-morbid conditions.</p></div><div><h3>Methods</h3><p>This is a retrospective cohort study of patients admitted between July 2010 and June 2015 at 651 US hospitals with a principal diagnosis of either pneumonia or secondary diagnosis of pneumonia with a primary diagnosis of respiratory failure or sepsis. Comorbidities were identified by ICD-9 codes and medical management by daily charge codes. Patients were categorized according to the presence and acuity of admission diagnosis of HF. In-hospital mortality was the primary outcome. Secondary outcomes included length of stay, hospital cost, ICU admission, use of mechanical ventilation, vasopressors and inotropes. Logistic regression was used to study the association of outcomes with presence and acuity of HF.</p></div><div><h3>Results</h3><p>Of 783,702 patients who met inclusion criteria, 212,203 (27%) had a diagnosis of HF. Of these, 56,306 (26.5%) had acute while 48,188 (22.7%) had chronic HF on admission; 51% had a diagnosis of unspecified HF. In multivariable-adjusted models, having any HF was associated with increased mortality (OR 1.35 [1.33 - 1.38]) compared to those without HF; increased mortality was associated with acute HF (OR 1.19 [1.15 - 1.22]) but not chronic HF (OR 0.92 [0.89 - 0.96]).</p></div><div><h3>Conclusion</h3><p>The worse outcomes for pneumonia patients with HF appear due to acute HF exacerbations. Adjustment for HF without accounting for chronicity could lead to biased prognostic and billing estimates.</p></div>","PeriodicalId":72168,"journal":{"name":"American journal of medicine open","volume":"7 ","pages":"Article 100013"},"PeriodicalIF":0.0000,"publicationDate":"2022-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/83/8c/nihms-1812932.PMC9211036.pdf","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"American journal of medicine open","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2667036422000073","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 1
Abstract
Background
Among patients admitted for pneumonia, heart failure (HF) is associated with worse outcomes. It is unclear whether this association is due to acute HF exacerbations, complex medical management, or chronic co-morbid conditions.
Methods
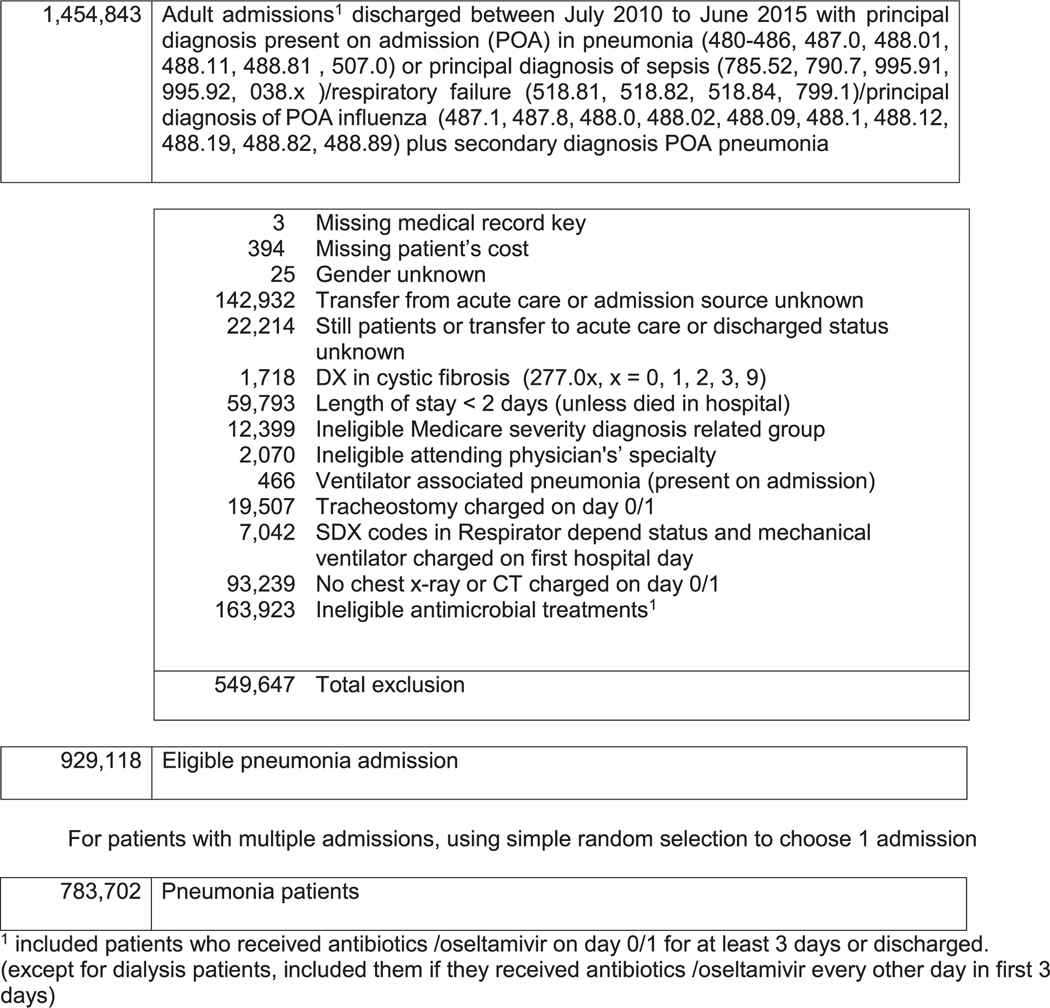
This is a retrospective cohort study of patients admitted between July 2010 and June 2015 at 651 US hospitals with a principal diagnosis of either pneumonia or secondary diagnosis of pneumonia with a primary diagnosis of respiratory failure or sepsis. Comorbidities were identified by ICD-9 codes and medical management by daily charge codes. Patients were categorized according to the presence and acuity of admission diagnosis of HF. In-hospital mortality was the primary outcome. Secondary outcomes included length of stay, hospital cost, ICU admission, use of mechanical ventilation, vasopressors and inotropes. Logistic regression was used to study the association of outcomes with presence and acuity of HF.
Results
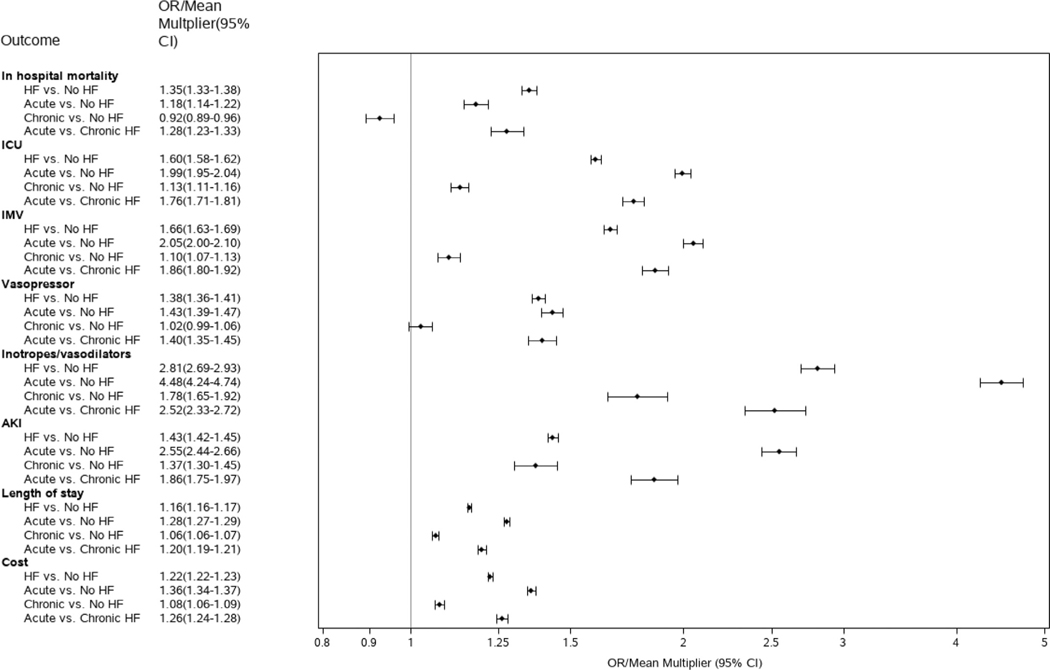
Of 783,702 patients who met inclusion criteria, 212,203 (27%) had a diagnosis of HF. Of these, 56,306 (26.5%) had acute while 48,188 (22.7%) had chronic HF on admission; 51% had a diagnosis of unspecified HF. In multivariable-adjusted models, having any HF was associated with increased mortality (OR 1.35 [1.33 - 1.38]) compared to those without HF; increased mortality was associated with acute HF (OR 1.19 [1.15 - 1.22]) but not chronic HF (OR 0.92 [0.89 - 0.96]).
Conclusion
The worse outcomes for pneumonia patients with HF appear due to acute HF exacerbations. Adjustment for HF without accounting for chronicity could lead to biased prognostic and billing estimates.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
