Dual Trigger with Gonadotropin Releasing Hormone Agonist and Human Chorionic Gonadotropin of Fresh Autologous Cycles in High Responders: A Systematic Review.
Andreas A Vyrides, Essam El Mahdi, Demetris Lamnisos, Konstantinos Giannakou
{"title":"Dual Trigger with Gonadotropin Releasing Hormone Agonist and Human Chorionic Gonadotropin of Fresh Autologous Cycles in High Responders: A Systematic Review.","authors":"Andreas A Vyrides, Essam El Mahdi, Demetris Lamnisos, Konstantinos Giannakou","doi":"10.18502/jri.v23i1.8446","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The purpose of the current study was to investigate the effect of co-administration of human chorionic gonadotropin (hCG) with gonadotropin releasing hormone agonist (GnRH-a) trigger (dual trigger) in high responders for fresh autologous cycles in order to investigate the pregnancy outcomes and rates of ovarian hyperstimulation syndrome (OHSS) in comparison to GnRH-a trigger alone.</p><p><strong>Methods: </strong>A systematic search was performed in PubMed and Ovid MEDLINE from inception through February 2020. The included materials were case-control, cohort and, cross-sectional studies as well as clinical trials in which the outcomes of dual trigger with GnRH-a were compared for final oocyte maturation in high responders undergoing GnRH-ant cycles.</p><p><strong>Results: </strong>Five retrospective studies were included for this review. Three of the studies showed that the use of dual trigger versus GnRH-a trigger resulted in no statistically significant difference in rates of OHSS while achieving a statistically significant difference in favor of the dual trigger group in ongoing pregnancy rates, early pregnancy loss, and fertilization rates.</p><p><strong>Conclusion: </strong>Currently, there is insufficient evidence to support improved clinical pregnancy rate, fertilization rate, live birth rate, and early pregnancy loss rate by the use of dual trigger versus GnRH-a trigger. Larger double-blind clinical studies are required to properly evaluate the efficacy of this protocol for use in high responders.</p>","PeriodicalId":38826,"journal":{"name":"Journal of Reproduction and Infertility","volume":"23 1","pages":"3-17"},"PeriodicalIF":0.0000,"publicationDate":"2022-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/24/d1/JRI-23-3.PMC9361727.pdf","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Reproduction and Infertility","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.18502/jri.v23i1.8446","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 1
Abstract
Background: The purpose of the current study was to investigate the effect of co-administration of human chorionic gonadotropin (hCG) with gonadotropin releasing hormone agonist (GnRH-a) trigger (dual trigger) in high responders for fresh autologous cycles in order to investigate the pregnancy outcomes and rates of ovarian hyperstimulation syndrome (OHSS) in comparison to GnRH-a trigger alone.
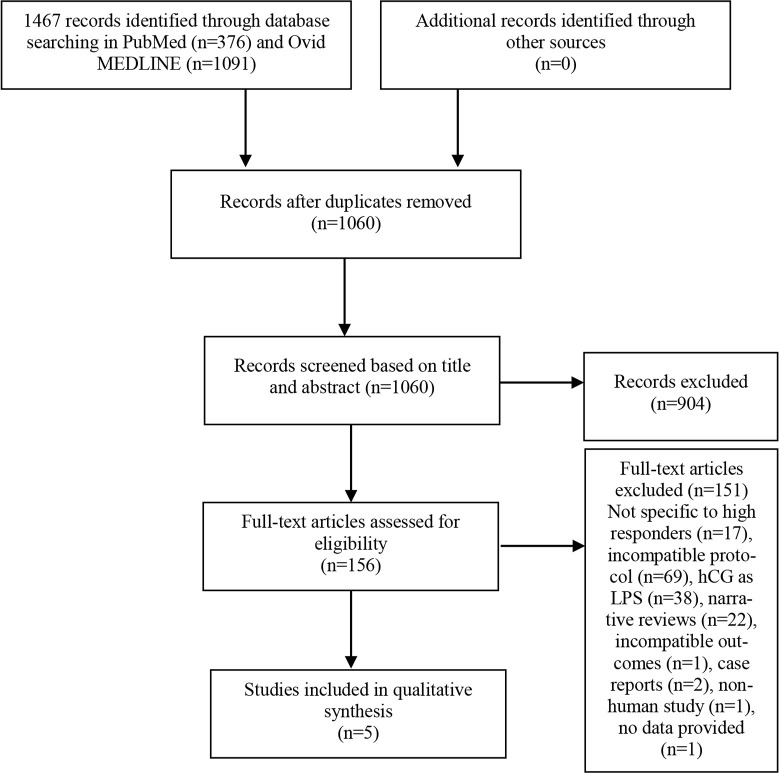
Methods: A systematic search was performed in PubMed and Ovid MEDLINE from inception through February 2020. The included materials were case-control, cohort and, cross-sectional studies as well as clinical trials in which the outcomes of dual trigger with GnRH-a were compared for final oocyte maturation in high responders undergoing GnRH-ant cycles.
Results: Five retrospective studies were included for this review. Three of the studies showed that the use of dual trigger versus GnRH-a trigger resulted in no statistically significant difference in rates of OHSS while achieving a statistically significant difference in favor of the dual trigger group in ongoing pregnancy rates, early pregnancy loss, and fertilization rates.
Conclusion: Currently, there is insufficient evidence to support improved clinical pregnancy rate, fertilization rate, live birth rate, and early pregnancy loss rate by the use of dual trigger versus GnRH-a trigger. Larger double-blind clinical studies are required to properly evaluate the efficacy of this protocol for use in high responders.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
