Vincent Issac Lau, Jeffrey A Johnson, Sean M Bagshaw, Oleksa G Rewa, John Basmaji, Kimberley A Lewis, M Elizabeth Wilcox, Kali Barrett, Francois Lamontagne, Francois Lauzier, Niall D Ferguson, Simon J W Oczkowski, Kirsten M Fiest, Daniel J Niven, Henry T Stelfox, Waleed Alhazzani, Margaret Herridge, Robert Fowler, Deborah J Cook, Bram Rochwerg, Feng Xie
{"title":"Health-related quality-of-life and health-utility reporting in critical care.","authors":"Vincent Issac Lau, Jeffrey A Johnson, Sean M Bagshaw, Oleksa G Rewa, John Basmaji, Kimberley A Lewis, M Elizabeth Wilcox, Kali Barrett, Francois Lamontagne, Francois Lauzier, Niall D Ferguson, Simon J W Oczkowski, Kirsten M Fiest, Daniel J Niven, Henry T Stelfox, Waleed Alhazzani, Margaret Herridge, Robert Fowler, Deborah J Cook, Bram Rochwerg, Feng Xie","doi":"10.5492/wjccm.v11.i4.236","DOIUrl":null,"url":null,"abstract":"<p><p>Mortality is a well-established patient-important outcome in critical care studies. In contrast, morbidity is less uniformly reported (given the myriad of critical care illnesses and complications of each) but may have a common end-impact on a patient's functional capacity and health-related quality-of-life (HRQoL). Survival with a poor quality-of-life may not be acceptable depending on individual patient values and preferences. Hence, as mortality decreases within critical care, it becomes increasingly important to measure intensive care unit (ICU) survivor HRQoL. HRQoL measurements with a preference-based scoring algorithm can be converted into health utilities on a scale anchored at 0 (representing death) and 1 (representing full health). They can be combined with survival to calculate quality-adjusted life-years (QALY), which are one of the most widely used methods of combining morbidity and mortality into a composite outcome. Although QALYs have been use for health-technology assessment decision-making, an emerging and novel role would be to inform clinical decision-making for patients, families and healthcare providers about what expected HRQoL may be during and after ICU care. Critical care randomized control trials (RCTs) have not routinely measured or reported HRQoL (until more recently), likely due to incapacity of some patients to participate in patient-reported outcome measures. Further differences in HRQoL measurement tools can lead to non-comparable values. To this end, we propose the validation of a gold-standard HRQoL tool in critical care, specifically the EQ-5D-5L. Both combined health-utility and mortality (disaggregated) and QALYs (aggregated) can be reported, with disaggregation allowing for determination of which components are the main drivers of the QALY outcome. Increased use of HRQoL, health-utility, and QALYs in critical care RCTs has the potential to: (1) Increase the likelihood of finding important effects if they exist; (2) improve research efficiency; and (3) help inform optimal management of critically ill patients allowing for decision-making about their HRQoL, in additional to traditional health-technology assessments.</p>","PeriodicalId":66959,"journal":{"name":"世界危重病急救学杂志(英文版)","volume":"11 4","pages":"236-245"},"PeriodicalIF":0.0000,"publicationDate":"2022-07-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/5e/19/WJCCM-11-236.PMC9305682.pdf","citationCount":"3","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"世界危重病急救学杂志(英文版)","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5492/wjccm.v11.i4.236","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 3
Abstract
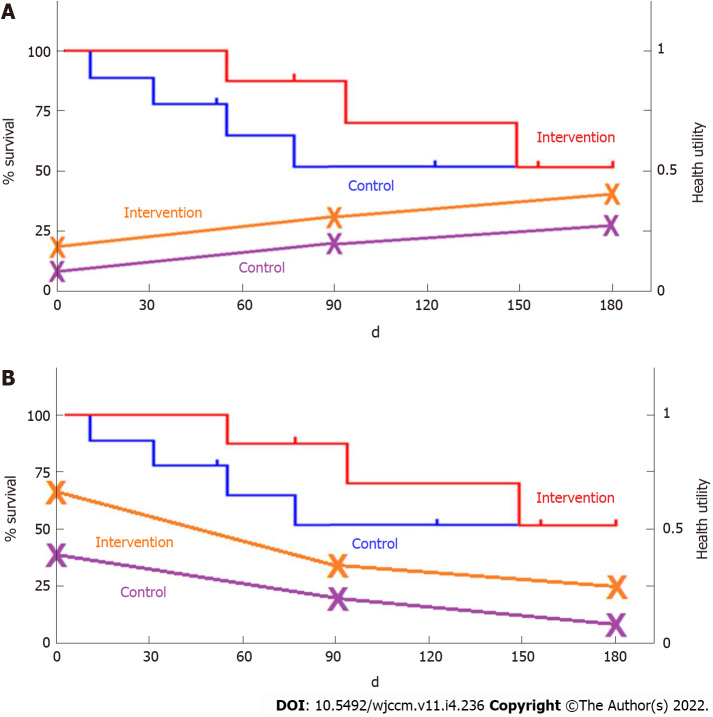
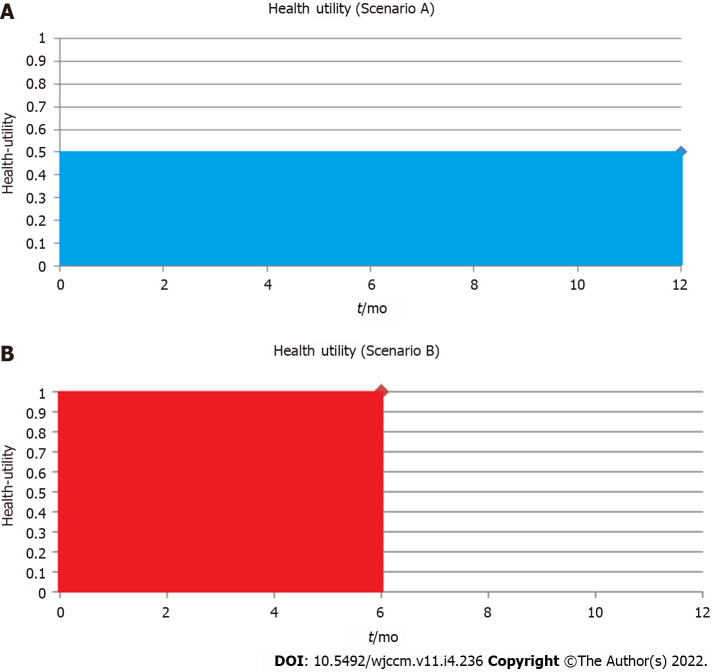
Mortality is a well-established patient-important outcome in critical care studies. In contrast, morbidity is less uniformly reported (given the myriad of critical care illnesses and complications of each) but may have a common end-impact on a patient's functional capacity and health-related quality-of-life (HRQoL). Survival with a poor quality-of-life may not be acceptable depending on individual patient values and preferences. Hence, as mortality decreases within critical care, it becomes increasingly important to measure intensive care unit (ICU) survivor HRQoL. HRQoL measurements with a preference-based scoring algorithm can be converted into health utilities on a scale anchored at 0 (representing death) and 1 (representing full health). They can be combined with survival to calculate quality-adjusted life-years (QALY), which are one of the most widely used methods of combining morbidity and mortality into a composite outcome. Although QALYs have been use for health-technology assessment decision-making, an emerging and novel role would be to inform clinical decision-making for patients, families and healthcare providers about what expected HRQoL may be during and after ICU care. Critical care randomized control trials (RCTs) have not routinely measured or reported HRQoL (until more recently), likely due to incapacity of some patients to participate in patient-reported outcome measures. Further differences in HRQoL measurement tools can lead to non-comparable values. To this end, we propose the validation of a gold-standard HRQoL tool in critical care, specifically the EQ-5D-5L. Both combined health-utility and mortality (disaggregated) and QALYs (aggregated) can be reported, with disaggregation allowing for determination of which components are the main drivers of the QALY outcome. Increased use of HRQoL, health-utility, and QALYs in critical care RCTs has the potential to: (1) Increase the likelihood of finding important effects if they exist; (2) improve research efficiency; and (3) help inform optimal management of critically ill patients allowing for decision-making about their HRQoL, in additional to traditional health-technology assessments.


 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
