Ciaran M Fairman, Simon Lønbro, Thomas D Cardaci, Brandon N VanderVeen, Tormod S Nilsen, Angela E Murphy
{"title":"Muscle wasting in cancer: opportunities and challenges for exercise in clinical cancer trials.","authors":"Ciaran M Fairman, Simon Lønbro, Thomas D Cardaci, Brandon N VanderVeen, Tormod S Nilsen, Angela E Murphy","doi":"10.1002/rco2.56","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Low muscle in cancer is associated with an increase in treatment-related toxicities and is a predictor of cancer-related and all-cause mortality. The mechanisms of cancer-related muscle loss are multifactorial, including anorexia, hypogonadism, anaemia, inflammation, malnutrition, and aberrations in skeletal muscle protein turnover and metabolism.</p><p><strong>Methods: </strong>In this narrative review, we summarise relevant literature to (i) review the factors influencing skeletal muscle mass regulation, (ii) provide an overview of how cancer/treatments negatively impact these, (iii) review factors beyond muscle signalling that can impact the ability to participate in and respond to an exercise intervention to counteract muscle loss in cancer, and (iv) provide perspectives on critical areas of future research.</p><p><strong>Results: </strong>Despite the well-known benefits of exercise, there remains a paucity of clinical evidence supporting the impact of exercise in cancer-related muscle loss. There are numerous challenges to reversing muscle loss with exercise in clinical cancer settings, ranging from the impact of cancer/treatments on the molecular regulation of muscle mass, to clinical challenges in responsiveness to an exercise intervention. For example, tumour-related/treatment-related factors (e.g. nausea, pain, anaemia, and neutropenia), presence of comorbidities (e.g. diabetes, arthritis, and chronic obstructive pulmonary disease), injuries, disease progression and bone metastases, concomitant medications (e.g., metformin), can negatively affect an individual's ability to exercise safely and limit subsequent adaptation.</p><p><strong>Conclusions: </strong>This review identifies numerous gaps and oppportunities in the area of low muscle and muscle loss in cancer. Collaborative efforts between preclinical and clinical researchers are imperative to both understanding the mechanisms of atrophy, and develop appropriate therapeutic interventions.</p>","PeriodicalId":73544,"journal":{"name":"JCSM rapid communications","volume":" ","pages":"52-67"},"PeriodicalIF":0.0000,"publicationDate":"2022-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9481195/pdf/","citationCount":"8","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JCSM rapid communications","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1002/rco2.56","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/12/22 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 8
Abstract
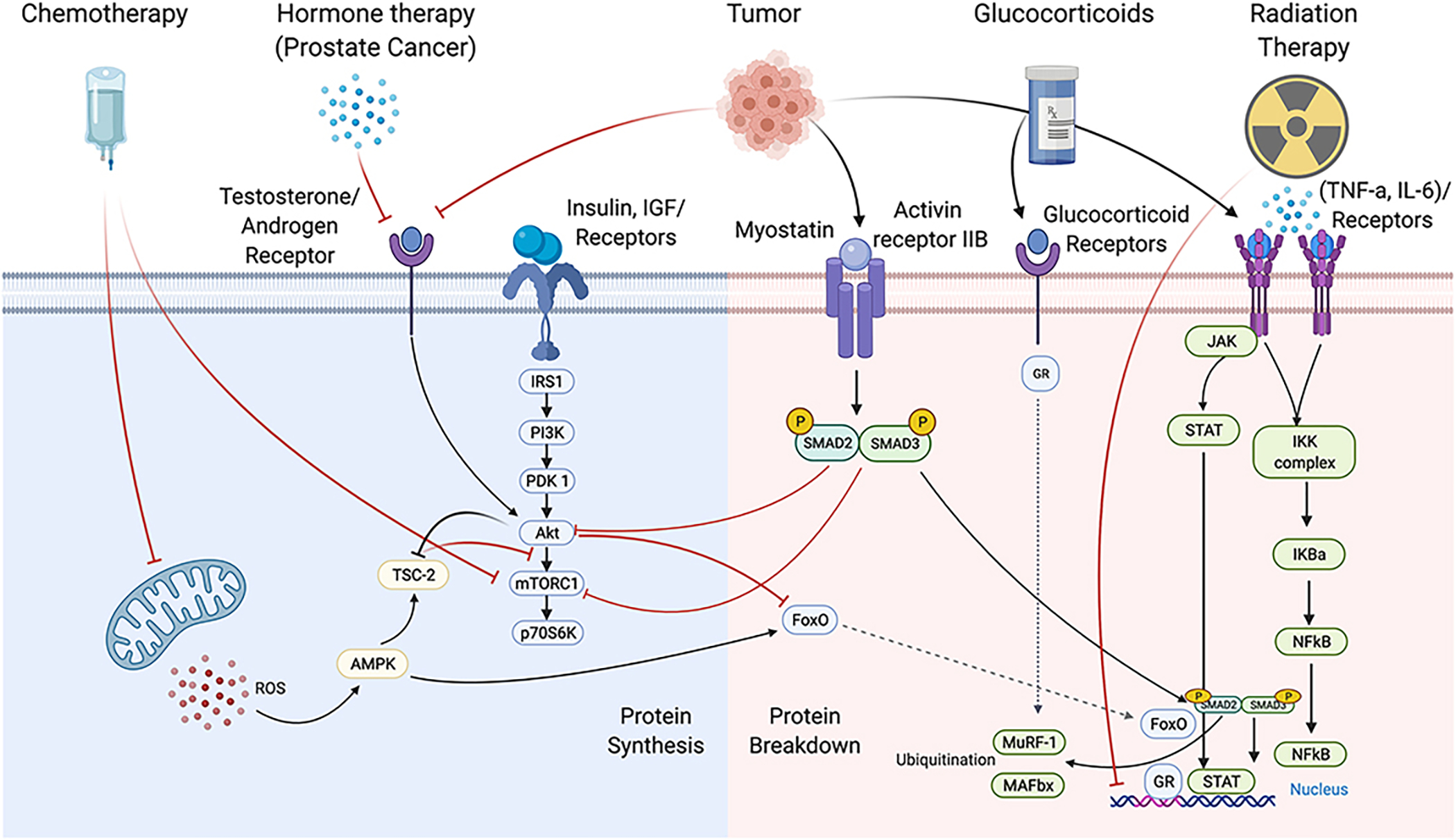
Background: Low muscle in cancer is associated with an increase in treatment-related toxicities and is a predictor of cancer-related and all-cause mortality. The mechanisms of cancer-related muscle loss are multifactorial, including anorexia, hypogonadism, anaemia, inflammation, malnutrition, and aberrations in skeletal muscle protein turnover and metabolism.
Methods: In this narrative review, we summarise relevant literature to (i) review the factors influencing skeletal muscle mass regulation, (ii) provide an overview of how cancer/treatments negatively impact these, (iii) review factors beyond muscle signalling that can impact the ability to participate in and respond to an exercise intervention to counteract muscle loss in cancer, and (iv) provide perspectives on critical areas of future research.
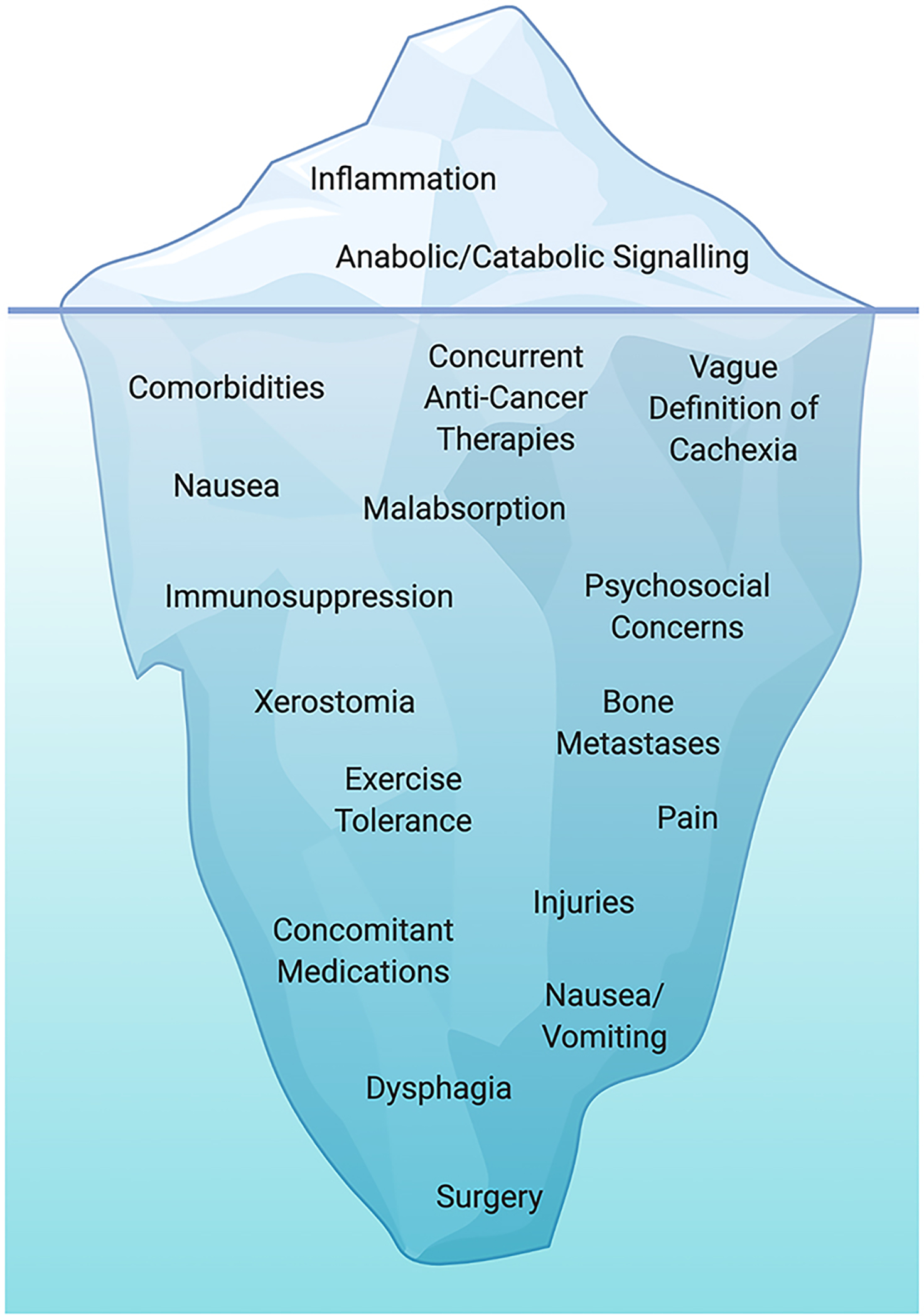
Results: Despite the well-known benefits of exercise, there remains a paucity of clinical evidence supporting the impact of exercise in cancer-related muscle loss. There are numerous challenges to reversing muscle loss with exercise in clinical cancer settings, ranging from the impact of cancer/treatments on the molecular regulation of muscle mass, to clinical challenges in responsiveness to an exercise intervention. For example, tumour-related/treatment-related factors (e.g. nausea, pain, anaemia, and neutropenia), presence of comorbidities (e.g. diabetes, arthritis, and chronic obstructive pulmonary disease), injuries, disease progression and bone metastases, concomitant medications (e.g., metformin), can negatively affect an individual's ability to exercise safely and limit subsequent adaptation.
Conclusions: This review identifies numerous gaps and oppportunities in the area of low muscle and muscle loss in cancer. Collaborative efforts between preclinical and clinical researchers are imperative to both understanding the mechanisms of atrophy, and develop appropriate therapeutic interventions.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
