{"title":"Pulsation of catheter during coronary angiography: Is it a sign of severe aortic regurgitation?","authors":"Muzaffer Kahyaoglu, Cetin Gecmen, Ozkan Candan","doi":"10.1556/1646.2020.00005","DOIUrl":null,"url":null,"abstract":"<p><p>A 48-year-old male patient was admitted to our outpatient clinic with complaints of shortness of breath. He also had a holo-diastolic murmur at the right sternal border and an apical impulse being displaced laterally and inferiorly. Transthoracic echocardiography showed a severe aortic regurgitation without aortic valve stenosis and a mildly dilated left ventricle accompanied by an ejection fraction of 55%. The aortic regurgitation jet was eccentric and there were significant holodiastolic flow reversals in the descending thoracic aorta. Surgical management was advised for this patient because of symptomatic severe aortic regurgitation. Then, the patient underwent preoperative coronary angiography through the right femoral artery route. The left coronary ostium could be engaged with a 6 Fr Judkins left diagnostic catheter; however, the catheter jumped through the ascending aorta. Afterwards, the catheter was engaged and again jumped through the ascending aorta. Engagement and jumping cycles observed between successive systole to diastole. In our opinion, this catheter movement is explained by wide pulse pressure, like the severe characteristic physical findings of severe aortic regurgitation. Further studies are needed to understand whether this catheter movement is angiographically evidence of severe aortic regurgitation.</p>","PeriodicalId":45181,"journal":{"name":"Interventional Medicine and Applied Science","volume":"11 4","pages":"221-223"},"PeriodicalIF":0.0000,"publicationDate":"2021-07-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/76/8d/imas-11-221.PMC9467382.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Interventional Medicine and Applied Science","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1556/1646.2020.00005","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/8/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
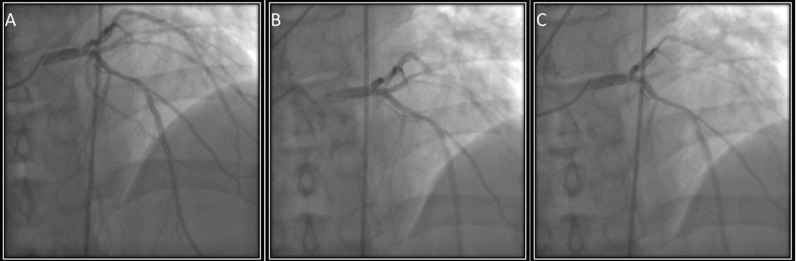
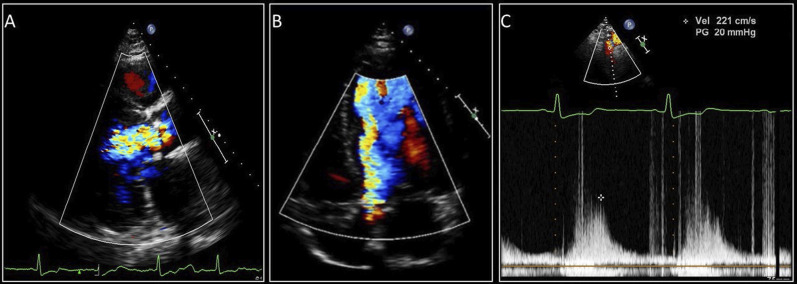
A 48-year-old male patient was admitted to our outpatient clinic with complaints of shortness of breath. He also had a holo-diastolic murmur at the right sternal border and an apical impulse being displaced laterally and inferiorly. Transthoracic echocardiography showed a severe aortic regurgitation without aortic valve stenosis and a mildly dilated left ventricle accompanied by an ejection fraction of 55%. The aortic regurgitation jet was eccentric and there were significant holodiastolic flow reversals in the descending thoracic aorta. Surgical management was advised for this patient because of symptomatic severe aortic regurgitation. Then, the patient underwent preoperative coronary angiography through the right femoral artery route. The left coronary ostium could be engaged with a 6 Fr Judkins left diagnostic catheter; however, the catheter jumped through the ascending aorta. Afterwards, the catheter was engaged and again jumped through the ascending aorta. Engagement and jumping cycles observed between successive systole to diastole. In our opinion, this catheter movement is explained by wide pulse pressure, like the severe characteristic physical findings of severe aortic regurgitation. Further studies are needed to understand whether this catheter movement is angiographically evidence of severe aortic regurgitation.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
