{"title":"Optimal timing for lung metastasectomy in patients with colorectal cancer.","authors":"Junji Ichinose, Kohei Hashimoto, Yosuke Matsuura, Masayuki Nakao, Takashi Akiyoshi, Yosuke Fukunaga, Sakae Okumura, Mingyon Mun","doi":"10.1093/icvts/ivac224","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>The possibility of occult metastasis remains a concern when deciding on lung metastasectomy. This study aimed to evaluate the utility of our two-step determination, which required confirmation that no new metastases had occurred over 3 months before surgery.</p><p><strong>Methods: </strong>Patients who were referred for colorectal lung metastases between 2007 and 2015 were reviewed. Immediate wedge resection was performed for cases with a single peripheral metastasis, whereas surgical indications for others were determined by the two-step determination. Early increase was defined as the emergence of new metastases within 4 months after the diagnosis of lung metastases.</p><p><strong>Results: </strong>Among 369 patients included, 92 were unresectable upon initial diagnosis, and 74 with single peripheral metastasis underwent immediate wedge resection. Surgical indications for the remaining 203 patients were ascertained based on the two-step determination. Surgery was not indicated in 48 patients (24%) due to new metastases or a favourable response to chemotherapy, with a median waiting duration of 4.8 months. Those who did not receive surgery had a worse prognosis than those who did (5-year overall survival: 21% vs 69%, P < 0.001) and were comparable to the initially unresectable group (5-year overall survival: 23%). Thirty-eight patients with early increase had lower surgical resection rates and worse prognoses than those without. Multivariable analysis identified early increase as an independent prognostic factor (hazard ratio: 4.49, P < 0.001).</p><p><strong>Conclusions: </strong>Patients with colorectal lung metastasis who developed new metastasis during the waiting period exhibited poor prognosis, suggesting the utility of the two-step determination of surgical indications.</p>","PeriodicalId":13621,"journal":{"name":"Interactive cardiovascular and thoracic surgery","volume":" ","pages":""},"PeriodicalIF":2.1000,"publicationDate":"2022-09-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9462424/pdf/","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Interactive cardiovascular and thoracic surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1093/icvts/ivac224","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 1
Abstract
Objectives: The possibility of occult metastasis remains a concern when deciding on lung metastasectomy. This study aimed to evaluate the utility of our two-step determination, which required confirmation that no new metastases had occurred over 3 months before surgery.
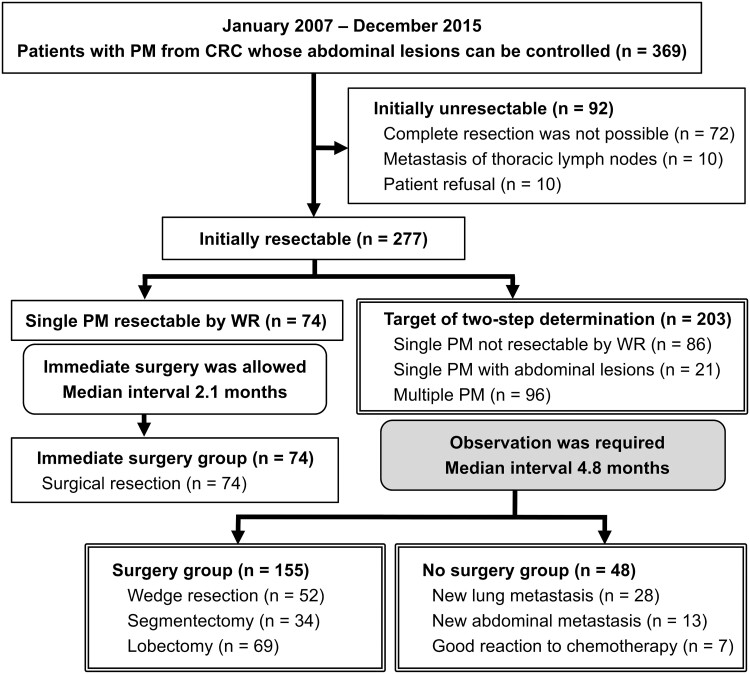
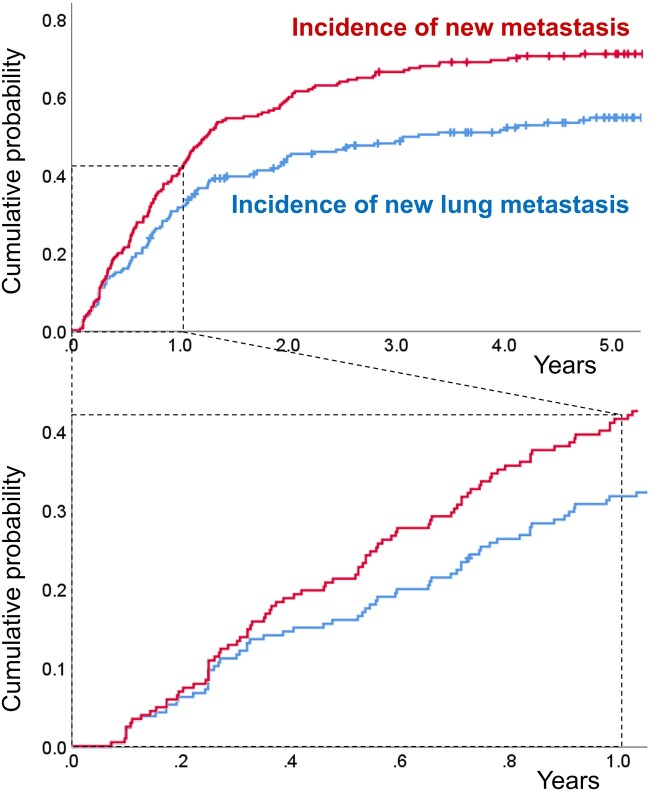
Methods: Patients who were referred for colorectal lung metastases between 2007 and 2015 were reviewed. Immediate wedge resection was performed for cases with a single peripheral metastasis, whereas surgical indications for others were determined by the two-step determination. Early increase was defined as the emergence of new metastases within 4 months after the diagnosis of lung metastases.
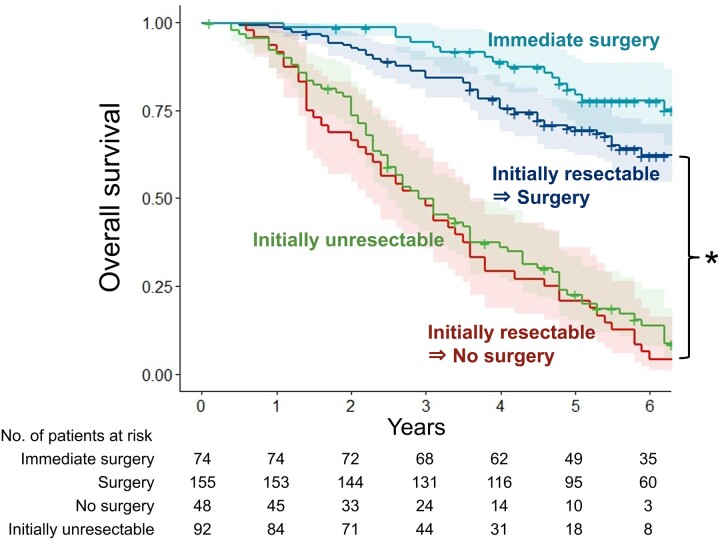
Results: Among 369 patients included, 92 were unresectable upon initial diagnosis, and 74 with single peripheral metastasis underwent immediate wedge resection. Surgical indications for the remaining 203 patients were ascertained based on the two-step determination. Surgery was not indicated in 48 patients (24%) due to new metastases or a favourable response to chemotherapy, with a median waiting duration of 4.8 months. Those who did not receive surgery had a worse prognosis than those who did (5-year overall survival: 21% vs 69%, P < 0.001) and were comparable to the initially unresectable group (5-year overall survival: 23%). Thirty-eight patients with early increase had lower surgical resection rates and worse prognoses than those without. Multivariable analysis identified early increase as an independent prognostic factor (hazard ratio: 4.49, P < 0.001).
Conclusions: Patients with colorectal lung metastasis who developed new metastasis during the waiting period exhibited poor prognosis, suggesting the utility of the two-step determination of surgical indications.
目的:在决定是否进行肺转移切除术时,隐匿性转移的可能性仍然是一个值得关注的问题。本研究旨在评估我们的两步测定方法的实用性,该方法需要在手术前3个月内确认没有新的转移灶发生。方法:回顾性分析2007年至2015年间转诊的结直肠肺转移患者。对于单个外周转移的病例,立即进行楔形切除,而其他病例的手术指征则由两步确定。早期增加定义为肺转移诊断后4个月内出现新的转移灶。结果:在369例患者中,92例初诊无法切除,74例单纯外周转移患者立即行楔形切除。其余203例患者采用两步确定手术指征。48例(24%)患者由于新的转移或对化疗的有利反应而不需要手术,中位等待时间为4.8个月。未接受手术的患者预后较接受手术的患者差(5年总生存率:21% vs 69%)。结论:在等待期出现新转移的结直肠癌肺转移患者预后较差,提示两步确定手术指征的实用性。
期刊介绍:
Interactive CardioVascular and Thoracic Surgery (ICVTS) publishes scientific contributions in the field of cardiovascular and thoracic surgery, covering all aspects of surgery of the heart, vessels and the chest. The journal publishes a range of article types including: Best Evidence Topics; Brief Communications; Case Reports; Original Articles; State-of-the-Art; Work in Progress Report.


 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
