Rate of Rehospitalization in 60 Days of Discharge and It's Determinants in Patients with Heart Failure with Reduced Ejection Fraction in a Tertiary Care Centre in India.
{"title":"Rate of Rehospitalization in 60 Days of Discharge and It's Determinants in Patients with Heart Failure with Reduced Ejection Fraction in a Tertiary Care Centre in India.","authors":"Kakasaheb H Bhosale, Ranjit Kumar Nath, Neeraj Pandit, Puneet Agarwal, Shripad Khairnar, Balram Yadav, Sulabh Chandrakar","doi":"10.36628/ijhf.2020.0007","DOIUrl":null,"url":null,"abstract":"<p><strong>Background and objectives: </strong>Identifying the patients with acute heart failure (HF) at high risk for rehospitalization after hospital discharge will enable proper optimization of treatment. This study is aimed to evaluate the rehospitalization rate at 60 days of discharge and their predictors in patients of chronic heart failure with reduced ejection fraction (HFrEF).</p><p><strong>Methods: </strong>This prospective observational study enrolled patients with left ventricle ejection fraction (LVEF) <40%, who were admitted because of acute decompensation. Patients were followed for 60 days to analyze rehospitalization rate and its predictors.</p><p><strong>Results: </strong>Of 103 HFrEF patients (74% male; mean age 55.8 years) enrolled, 7 patients died during index admission and 3 patients lost to follow up. The 60-day rehospitalization rate was 37% (34/93). We studied 23 clinical and 9 biochemical predictors of rehospitalization. Out of 34 events of rehospitalization, 79.41% (n=28) was due to cardiac cause followed by respiratory 5.8% (n=2), renal 5.8% (n=2) and others 5.8% (n=2). Among all the parameters, on logistic regression analysis having longer length of index hospital stay (>7 days) (52.8% vs. 28.8%; odds ratio [OR], 1.79; confidence interval [CI], 1.2-7.25; p=0.040) and chronic kidney disease (CKD) (26.5% vs. 8.5%; OR, 3.06; CI, 1.1-57.04; p=0.050) independently increased the risk of rehospitalization at 60 days of discharge. Further higher haemoglobin level (11.3 vs. 9.9 gm/dL; OR, 0.71; CI, 0.48-0.97; p=0.050) and higher LVEF at index admission (30.4% vs. 26.5%; OR, 0.87; CI, 0.75-0.99; p=0.049) were associated with decreased the risk of rehospitalization.</p><p><strong>Conclusions: </strong>Our study reveals that patients with HFrEF have significantly higher rehospitalization rate (37%) and in-hospital mortality rates (6.78%) of any chronic cardiac disease conditions. Correction of low hemoglobin and special care in those who are having very low LVEF, CKD and longer length of stay, including tailored therapy and frequent visits may play an important role in preventing future rehospitalization in these patients.</p>","PeriodicalId":14058,"journal":{"name":"International Journal of Heart Failure","volume":"2 2","pages":"131-144"},"PeriodicalIF":0.0000,"publicationDate":"2020-04-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/66/b2/ijhf-2-131.PMC9536659.pdf","citationCount":"8","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Journal of Heart Failure","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.36628/ijhf.2020.0007","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2020/4/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 8
Abstract
Background and objectives: Identifying the patients with acute heart failure (HF) at high risk for rehospitalization after hospital discharge will enable proper optimization of treatment. This study is aimed to evaluate the rehospitalization rate at 60 days of discharge and their predictors in patients of chronic heart failure with reduced ejection fraction (HFrEF).
Methods: This prospective observational study enrolled patients with left ventricle ejection fraction (LVEF) <40%, who were admitted because of acute decompensation. Patients were followed for 60 days to analyze rehospitalization rate and its predictors.
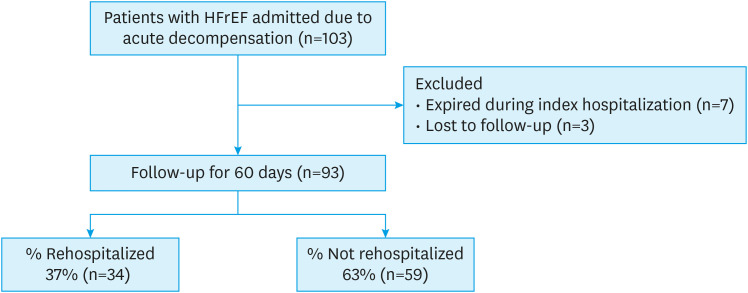
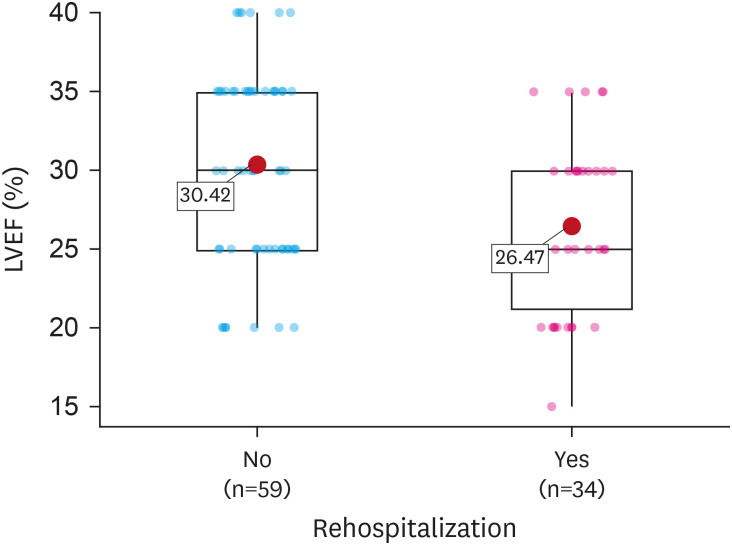
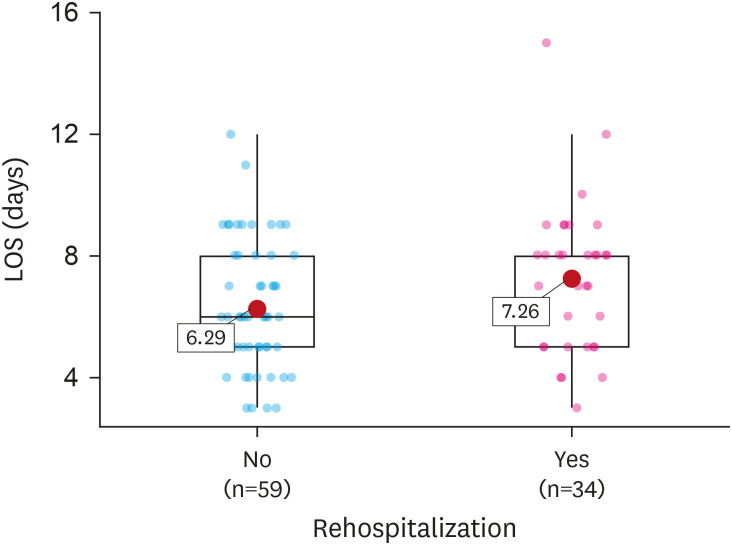
Results: Of 103 HFrEF patients (74% male; mean age 55.8 years) enrolled, 7 patients died during index admission and 3 patients lost to follow up. The 60-day rehospitalization rate was 37% (34/93). We studied 23 clinical and 9 biochemical predictors of rehospitalization. Out of 34 events of rehospitalization, 79.41% (n=28) was due to cardiac cause followed by respiratory 5.8% (n=2), renal 5.8% (n=2) and others 5.8% (n=2). Among all the parameters, on logistic regression analysis having longer length of index hospital stay (>7 days) (52.8% vs. 28.8%; odds ratio [OR], 1.79; confidence interval [CI], 1.2-7.25; p=0.040) and chronic kidney disease (CKD) (26.5% vs. 8.5%; OR, 3.06; CI, 1.1-57.04; p=0.050) independently increased the risk of rehospitalization at 60 days of discharge. Further higher haemoglobin level (11.3 vs. 9.9 gm/dL; OR, 0.71; CI, 0.48-0.97; p=0.050) and higher LVEF at index admission (30.4% vs. 26.5%; OR, 0.87; CI, 0.75-0.99; p=0.049) were associated with decreased the risk of rehospitalization.
Conclusions: Our study reveals that patients with HFrEF have significantly higher rehospitalization rate (37%) and in-hospital mortality rates (6.78%) of any chronic cardiac disease conditions. Correction of low hemoglobin and special care in those who are having very low LVEF, CKD and longer length of stay, including tailored therapy and frequent visits may play an important role in preventing future rehospitalization in these patients.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
