Treatment of Ischemic Stroke Following Intracranial Hemorrhage in a Patient with Continuous Flow Left Ventricular Assist Device: Between a Rock and a Hard Place.
Hee Jeong Lee, Yun Seok Kim, Woo Sung Jang, Keun Tae Kim, Chang-Hyun Kim, In-Cheol Kim
{"title":"Treatment of Ischemic Stroke Following Intracranial Hemorrhage in a Patient with Continuous Flow Left Ventricular Assist Device: Between a Rock and a Hard Place.","authors":"Hee Jeong Lee, Yun Seok Kim, Woo Sung Jang, Keun Tae Kim, Chang-Hyun Kim, In-Cheol Kim","doi":"10.36628/ijhf.2021.0034","DOIUrl":null,"url":null,"abstract":"A 75-year-old male with a continuous-flow left ventricular assist device (LVAD) was brought to the emergency room (ER) after losing consciousness due to head trauma following orthostatic dizziness. At the ER, non-contrast brain computed tomography (CT) showed no evidence of intracranial hemorrhage (Figure 1A and B), and the patient exhibited no neurological deficits. He had an LVAD (Heartware Ventricular Assist Device System; Medtronic Inc., Minnesota, MN, USA), implanted 14 months prior to presentation, due to ischemic cardiomyopathy. After successful LVAD treatment for the destination therapy, he was treated with aspirin and warfarin with an international normalized ratio (INR) target of 2–3. His vital signs and basic laboratory test results were normal, but the INR was slightly elevated at 3.43. The LVAD setting was stable with a revolution of 2,500/min, flow of 3.5 L/ min, and power of 3.2 watts. He was discharged with a decreased dose of warfarin from 4.5 mg to 4 mg. Five days later, the patient returned to the ER due to dysarthria. His INR was within the target range (2.86), and the LVAD function was stable (2,500/min, flow 3.3 L, power 3.2 watts). However, brain CT revealed multiple traumatic subarachnoid and intra-parenchymal hemorrhages (Figure 1). Vitamin K (10 mg) was immediately injected, and antithrombotic drugs (aspirin and warfarin) were discontinued. The target mean blood pressure was 65–80 mmHg. His symptoms improved, and a follow-up brain CT scan showed reduced hemorrhagic lesions. On the 16th post-admission day (PAD), he lost consciousness again. His vital signs and LVAD function (2,500/min, flow 3.1 L, power 3.1 watts) remained stable. Transthoracic echocardiography also showed no change in interval from the previous examination, and there was no evidence of intracardiac thrombosis. Brain CT angiography was performed instead of brain magnetic resonance imaging (MRI). It revealed total occlusion of the left middle cerebral artery (MCA) (Figure 2). During endovascular revascularization therapy, the total occlusion of the left MCA M2 segment was identified. The thrombectomy was successful, resulting in complete recanalization within 3 Int J Heart Fail. 2021 Oct;3(4):244-248 https://doi.org/10.36628/ijhf.2021.0034 pISSN 2636-154X·eISSN 2636-1558","PeriodicalId":14058,"journal":{"name":"International Journal of Heart Failure","volume":"3 4","pages":"244-248"},"PeriodicalIF":0.0000,"publicationDate":"2021-10-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/38/90/ijhf-3-244.PMC9536686.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Journal of Heart Failure","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.36628/ijhf.2021.0034","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/10/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
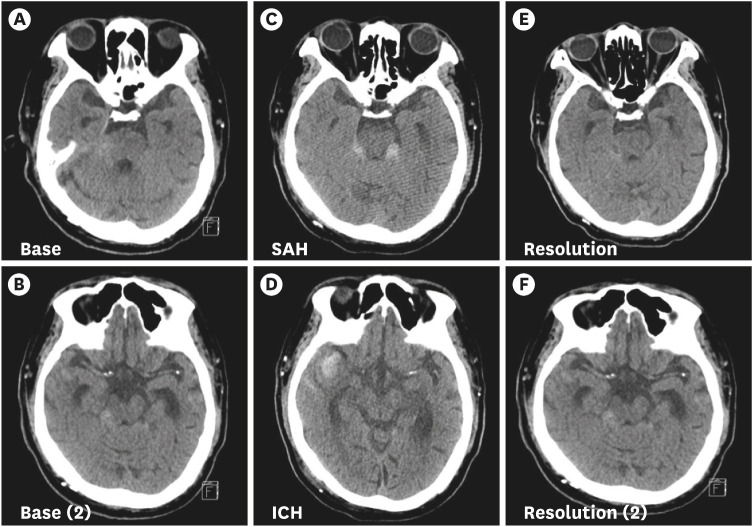
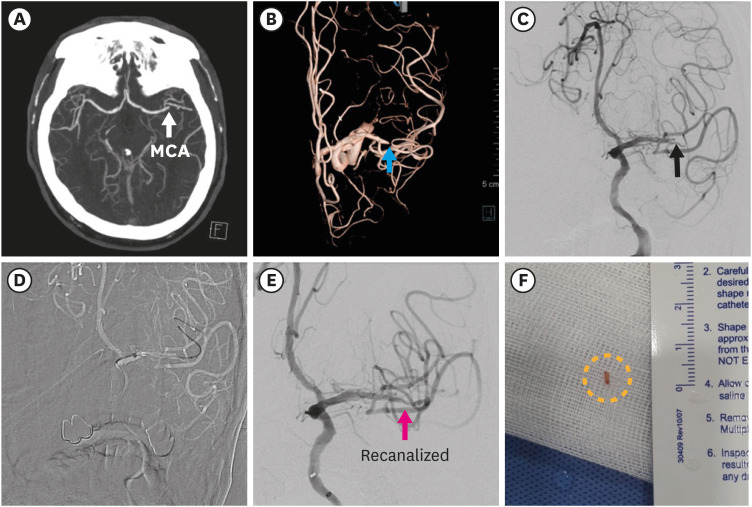
A 75-year-old male with a continuous-flow left ventricular assist device (LVAD) was brought to the emergency room (ER) after losing consciousness due to head trauma following orthostatic dizziness. At the ER, non-contrast brain computed tomography (CT) showed no evidence of intracranial hemorrhage (Figure 1A and B), and the patient exhibited no neurological deficits. He had an LVAD (Heartware Ventricular Assist Device System; Medtronic Inc., Minnesota, MN, USA), implanted 14 months prior to presentation, due to ischemic cardiomyopathy. After successful LVAD treatment for the destination therapy, he was treated with aspirin and warfarin with an international normalized ratio (INR) target of 2–3. His vital signs and basic laboratory test results were normal, but the INR was slightly elevated at 3.43. The LVAD setting was stable with a revolution of 2,500/min, flow of 3.5 L/ min, and power of 3.2 watts. He was discharged with a decreased dose of warfarin from 4.5 mg to 4 mg. Five days later, the patient returned to the ER due to dysarthria. His INR was within the target range (2.86), and the LVAD function was stable (2,500/min, flow 3.3 L, power 3.2 watts). However, brain CT revealed multiple traumatic subarachnoid and intra-parenchymal hemorrhages (Figure 1). Vitamin K (10 mg) was immediately injected, and antithrombotic drugs (aspirin and warfarin) were discontinued. The target mean blood pressure was 65–80 mmHg. His symptoms improved, and a follow-up brain CT scan showed reduced hemorrhagic lesions. On the 16th post-admission day (PAD), he lost consciousness again. His vital signs and LVAD function (2,500/min, flow 3.1 L, power 3.1 watts) remained stable. Transthoracic echocardiography also showed no change in interval from the previous examination, and there was no evidence of intracardiac thrombosis. Brain CT angiography was performed instead of brain magnetic resonance imaging (MRI). It revealed total occlusion of the left middle cerebral artery (MCA) (Figure 2). During endovascular revascularization therapy, the total occlusion of the left MCA M2 segment was identified. The thrombectomy was successful, resulting in complete recanalization within 3 Int J Heart Fail. 2021 Oct;3(4):244-248 https://doi.org/10.36628/ijhf.2021.0034 pISSN 2636-154X·eISSN 2636-1558


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
