Junho Hyun, Sang Eun Lee, Seung-Ah Lee, Jung Ae Hong, Min-Seok Kim, Jae-Joong Kim
{"title":"Rationale and Study Design of the Withdrawal of Spironolactone for Heart Failure with Improved Left Ventricular Ejection Fraction.","authors":"Junho Hyun, Sang Eun Lee, Seung-Ah Lee, Jung Ae Hong, Min-Seok Kim, Jae-Joong Kim","doi":"10.36628/ijhf.2020.0044","DOIUrl":null,"url":null,"abstract":"<p><p>It is unclear if guideline-directed medical therapy (GDMT) should be maintained in patients who have heart failure (HF) with improved ejection fraction (HFiEF). Of the medications recommended for HF, mineralocorticoid receptor antagonist (MRA) is associated with heterogeneous results and considerable adverse events. We wish to evaluate whether MRA withdrawal is safe or associated with deterioration of left ventricular ejection fraction (LVEF). We will select 60 patients with HFiEF of a New York Heart Association functional class I-II who are receiving GDMT and randomize them in a 1:1 fashion into 2 groups: one that will continue treatment and one that will have spironolactone administration withdrawn. All patients will receive standard medical therapy other than MRA. The primary outcome is the proportion of patients with declining LVEF ≥10%. Secondary outcomes include a change in LVEF, the estimated glomerular filtration rate, B-type natriuretic peptide or N-terminal pro-brain natriuretic peptide levels, and adverse clinical events, including death, re-hospitalization, or an emergency department visit for HF. This trial will provide important evidence on whether MRA in addition to other standard therapy, should be maintained or withdrawn in patients with HFiEF.</p>","PeriodicalId":14058,"journal":{"name":"International Journal of Heart Failure","volume":"3 1","pages":"51-58"},"PeriodicalIF":0.0000,"publicationDate":"2021-01-14","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/1a/e0/ijhf-3-51.PMC9536720.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Journal of Heart Failure","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.36628/ijhf.2020.0044","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
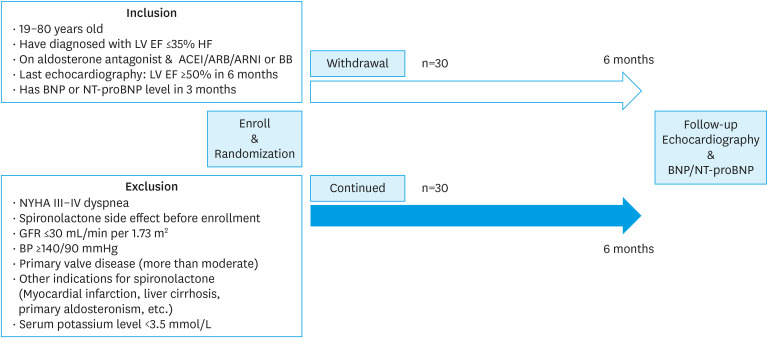
It is unclear if guideline-directed medical therapy (GDMT) should be maintained in patients who have heart failure (HF) with improved ejection fraction (HFiEF). Of the medications recommended for HF, mineralocorticoid receptor antagonist (MRA) is associated with heterogeneous results and considerable adverse events. We wish to evaluate whether MRA withdrawal is safe or associated with deterioration of left ventricular ejection fraction (LVEF). We will select 60 patients with HFiEF of a New York Heart Association functional class I-II who are receiving GDMT and randomize them in a 1:1 fashion into 2 groups: one that will continue treatment and one that will have spironolactone administration withdrawn. All patients will receive standard medical therapy other than MRA. The primary outcome is the proportion of patients with declining LVEF ≥10%. Secondary outcomes include a change in LVEF, the estimated glomerular filtration rate, B-type natriuretic peptide or N-terminal pro-brain natriuretic peptide levels, and adverse clinical events, including death, re-hospitalization, or an emergency department visit for HF. This trial will provide important evidence on whether MRA in addition to other standard therapy, should be maintained or withdrawn in patients with HFiEF.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
