Omar Toubat PhD , Li Ding MD, MPH , Keyue Ding PhD , Sean C. Wightman MD , Scott M. Atay MD , Takashi Harano MD , Anthony W. Kim MD , Elizabeth A. David MD, MAS
{"title":"Benefit of adjuvant chemotherapy for resected pathologic N1 non-small cell lung cancer is unrecognized: A subgroup analysis of the JBR10 trial","authors":"Omar Toubat PhD , Li Ding MD, MPH , Keyue Ding PhD , Sean C. Wightman MD , Scott M. Atay MD , Takashi Harano MD , Anthony W. Kim MD , Elizabeth A. David MD, MAS","doi":"10.1053/j.semtcvs.2022.10.005","DOIUrl":null,"url":null,"abstract":"<div><p><span>Adjuvant chemotherapy is underutilized in clinical practice, in part, because its anticipated survival benefit is limited. We evaluated the impact of AC on overall and recurrence-free survival among completely resected pN1 </span>NSCLC<span><span><span> patients enrolled in the North American Intergroup phase III (JBR10) trial. A post-hoc subgroup analysis of pN1 NSCLC patients was performed. Participants were randomized to cisplatin+vinorelbine (AC) (n = 118) or observation (n = 116) following complete resection. The primary endpoint was overall survival (OS). The secondary endpoint was recurrence free survival (RFS). Kaplan-Meier methods were used to compare OS and RFS between the two </span>treatment groups. </span>Cox regression was used to identify factors associated with OS and RFS endpoints. Both groups had similar baseline characteristics. AC patients had improved 5-year OS (AC 61.4% vs observation 41.0%, log-rank p = .008) and 5-year RFS (AC 56.2% vs observation 39.9%, log-rank p = .011) rates compared to observation. Cox regression analyses confirmed the OS (HR 0.583, 95% CI 0.402-0.846, p = .005) and RFS (HR 0.573, 95% CI 0.395-0.830, p = .003) benefit associated with AC. AC was associated with a lower risk (HR 0.648, 95% CI 0.435-0.965, p = .0326) and a lower cumulative incidence (Subdistribution Hazard Ratio [SHR], 0.67, 95% CI 0.449-0.999, p = .0498) of lung cancer deaths. In the JBR10 trial, treatment with AC conferred a significant OS and RFS advantage over observation for pN1 NSCLC patients. These data suggest that pN1 NSCLC patients may experience a disproportionately greater clinical benefit from AC than the 6% survival advantage estimated by the LACE meta-analysis.</span></p></div>","PeriodicalId":48592,"journal":{"name":"Seminars in Thoracic and Cardiovascular Surgery","volume":"36 2","pages":"Pages 261-270"},"PeriodicalIF":2.5000,"publicationDate":"2024-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Seminars in Thoracic and Cardiovascular Surgery","FirstCategoryId":"3","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S104306792200257X","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
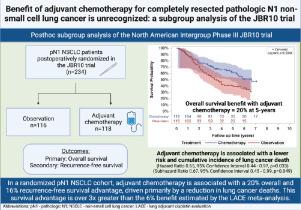
Adjuvant chemotherapy is underutilized in clinical practice, in part, because its anticipated survival benefit is limited. We evaluated the impact of AC on overall and recurrence-free survival among completely resected pN1 NSCLC patients enrolled in the North American Intergroup phase III (JBR10) trial. A post-hoc subgroup analysis of pN1 NSCLC patients was performed. Participants were randomized to cisplatin+vinorelbine (AC) (n = 118) or observation (n = 116) following complete resection. The primary endpoint was overall survival (OS). The secondary endpoint was recurrence free survival (RFS). Kaplan-Meier methods were used to compare OS and RFS between the two treatment groups. Cox regression was used to identify factors associated with OS and RFS endpoints. Both groups had similar baseline characteristics. AC patients had improved 5-year OS (AC 61.4% vs observation 41.0%, log-rank p = .008) and 5-year RFS (AC 56.2% vs observation 39.9%, log-rank p = .011) rates compared to observation. Cox regression analyses confirmed the OS (HR 0.583, 95% CI 0.402-0.846, p = .005) and RFS (HR 0.573, 95% CI 0.395-0.830, p = .003) benefit associated with AC. AC was associated with a lower risk (HR 0.648, 95% CI 0.435-0.965, p = .0326) and a lower cumulative incidence (Subdistribution Hazard Ratio [SHR], 0.67, 95% CI 0.449-0.999, p = .0498) of lung cancer deaths. In the JBR10 trial, treatment with AC conferred a significant OS and RFS advantage over observation for pN1 NSCLC patients. These data suggest that pN1 NSCLC patients may experience a disproportionately greater clinical benefit from AC than the 6% survival advantage estimated by the LACE meta-analysis.
期刊介绍:
Seminars in Thoracic and Cardiovascular Surgery is devoted to providing a forum for cardiothoracic surgeons to disseminate and discuss important new information and to gain insight into unresolved areas of question in the specialty. Each issue presents readers with a selection of original peer-reviewed articles accompanied by editorial commentary from specialists in the field. In addition, readers are offered valuable invited articles: State of Views editorials and Current Readings highlighting the latest contributions on central or controversial issues. Another prized feature is expert roundtable discussions in which experts debate critical questions for cardiothoracic treatment and care. Seminars is an invitation-only publication that receives original submissions transferred ONLY from its sister publication, The Journal of Thoracic and Cardiovascular Surgery. As we continue to expand the reach of the Journal, we will explore the possibility of accepting unsolicited manuscripts in the future.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
