Soo-Jin Kim, Bong-Joon Kim, Sung-Il Im, Hyun-Su Kim, Jung-Ho Heo
{"title":"Effects of Empagliflozin on Diuretics Reduction in Outpatient Heart Failure Patients.","authors":"Soo-Jin Kim, Bong-Joon Kim, Sung-Il Im, Hyun-Su Kim, Jung-Ho Heo","doi":"10.36628/ijhf.2022.0009","DOIUrl":null,"url":null,"abstract":"<p><strong>Background and objectives: </strong>Inhibitors of sodium-glucose cotransporter 2 (SGLT2i) reduce the risk of hospitalization for heart failure (HF). We aimed to examine the effect of empagliflozin on change of diuretics dose in outpatient HF patients.</p><p><strong>Methods: </strong>We retrospectively reviewed the medical records of 612 patients who were treated using both empagliflozin and diuretics. We excluded patients who did not meet the criteria for HF. Dose and duration of empagliflozin and diuretics were measured.</p><p><strong>Results: </strong>Of 612 patients, a total of 251 was analyzed and followed for a mean 430.0±175.4 days. The mean age was 69.3, 51.8% were female, and 93.2% had type 2 diabetes. The distribution of initial diuretics type when starting empagliflozin showed that furosemide comprised 24.7%, spironolactone 20.7%, thiazide 36.9%, and others. Total 23.1% of patients reduced diuretic dose, 13.1% increased diuretic dose, 41.4% continued at the same diuretic dose, and 22.3% switched to different diuretics. Among patients who were using furosemide, 36.0% reduced diuretics dose. There was a diuretic reduction in 22.6% of HF preserved ejection fraction (HFpEF, left ventricular ejection fraction [LVEF] ≥50%) and in 26.5% of HF reduced EF (HFrEF, LVEF <50%). The average doses furosemide at the start of empagliflozin decreased from 16.3mg/day to 8.5mg/day at the time of follow-up.</p><p><strong>Conclusions: </strong>Among outpatient clinic HF patients treated with both diuretics and empagliflozin, 23.1% of patients had their diuretics reduced, and the mean dose of furosemide was reduced by about half. This suggests that empagliflozin has clinical advantages in managing outpatient HF patients.</p>","PeriodicalId":14058,"journal":{"name":"International Journal of Heart Failure","volume":"4 4","pages":"183-192"},"PeriodicalIF":0.0000,"publicationDate":"2022-07-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/a0/c0/ijhf-4-183.PMC9634028.pdf","citationCount":"5","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Journal of Heart Failure","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.36628/ijhf.2022.0009","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/10/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 5
Abstract
Background and objectives: Inhibitors of sodium-glucose cotransporter 2 (SGLT2i) reduce the risk of hospitalization for heart failure (HF). We aimed to examine the effect of empagliflozin on change of diuretics dose in outpatient HF patients.
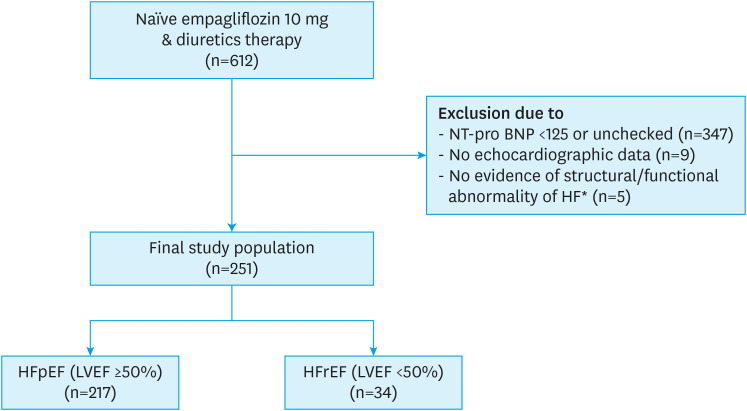
Methods: We retrospectively reviewed the medical records of 612 patients who were treated using both empagliflozin and diuretics. We excluded patients who did not meet the criteria for HF. Dose and duration of empagliflozin and diuretics were measured.
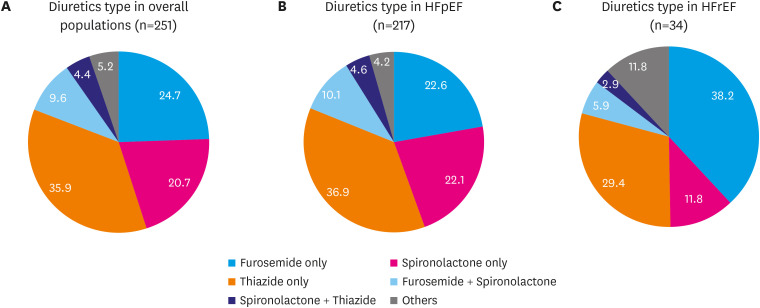
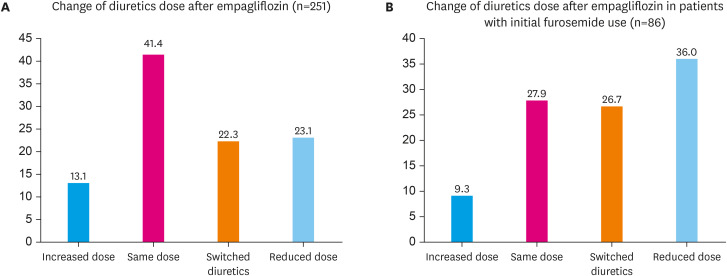
Results: Of 612 patients, a total of 251 was analyzed and followed for a mean 430.0±175.4 days. The mean age was 69.3, 51.8% were female, and 93.2% had type 2 diabetes. The distribution of initial diuretics type when starting empagliflozin showed that furosemide comprised 24.7%, spironolactone 20.7%, thiazide 36.9%, and others. Total 23.1% of patients reduced diuretic dose, 13.1% increased diuretic dose, 41.4% continued at the same diuretic dose, and 22.3% switched to different diuretics. Among patients who were using furosemide, 36.0% reduced diuretics dose. There was a diuretic reduction in 22.6% of HF preserved ejection fraction (HFpEF, left ventricular ejection fraction [LVEF] ≥50%) and in 26.5% of HF reduced EF (HFrEF, LVEF <50%). The average doses furosemide at the start of empagliflozin decreased from 16.3mg/day to 8.5mg/day at the time of follow-up.
Conclusions: Among outpatient clinic HF patients treated with both diuretics and empagliflozin, 23.1% of patients had their diuretics reduced, and the mean dose of furosemide was reduced by about half. This suggests that empagliflozin has clinical advantages in managing outpatient HF patients.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
