Fowzia Ibrahim, Ian C Scott, David L Scott, Salma Ahmed Ayis
{"title":"Heterogeneity of treatment responses in rheumatoid arthritis using group based trajectory models: secondary analysis of clinical trial data.","authors":"Fowzia Ibrahim, Ian C Scott, David L Scott, Salma Ahmed Ayis","doi":"10.1186/s41927-023-00348-5","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Traditionally rheumatoid arthritis (RA) trials classify patients as responders and non-responders; they ignore the potential range of treatment responses. Group Based Trajectory Models (GBTMs) provide a more refined approach. They identify patient subgroups with similar outcome trajectories. We used GBTMs to classify patients into subgroups of varying responses and explore factors associated with different responses to intensive treatment in a secondary analysis of intensive treatment in the TITRATE clinical trial.</p><p><strong>Methods: </strong>The TITRATE trial enrolled 335 patients with RA: 168 patients were randomised to receive intensive management, which comprised monthly assessments including measures of the disease activity score for 28 joints (DAS28), treatment escalation when patients were not responding sufficiently and psychosocial support; 163 of these patients completed the trial. We applied GBTMs to monthly DAS28 scores over one year to these patients who had received intensive management. The control group had standard care and were assessed every 6 months; they had too few DAS28 scores for applying GBTMs.</p><p><strong>Results: </strong>GBTMs identified three distinct trajectories in the patients receiving intensive management: good (n = 40), moderate (n = 76) and poor (n = 47) responders. Baseline body mass index (BMI), disability, fatigue and depression levels were significantly different between trajectory groups. Few (10%) good responders were obese, compared to 38% of moderate, and 43% of poor responders (P = 0.002). Few (8%) good responders had depression, compared to 14% moderate responders, and 38% poor responders (P < 0.001). The key difference in treatments was using high-cost biologics, used in only 5% of good responders but 30% of moderate and 51% of poor responders (P < 0.001). Most good responders had endpoint remissions and low disability, pain, and fatigue scores; few poor responders achieved any favourable outcomes.</p><p><strong>Conclusion: </strong>GBTMs identified three trajectories of disease activity progression in patients receiving intensive management for moderately active RA. Baseline variables like obesity and depression predicted different treatment responses. Few good responders needed biologic drugs; they responded to conventional DMARDs alone. GBTMs have the potential to facilitate precision medicine enabling patient-oriented treatment strategies based on key characteristics.</p><p><strong>Registration: </strong>TITRATE Trial ISRCTN 70160382.</p>","PeriodicalId":9150,"journal":{"name":"BMC Rheumatology","volume":"7 1","pages":"33"},"PeriodicalIF":2.5000,"publicationDate":"2023-09-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10518927/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMC Rheumatology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s41927-023-00348-5","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"RHEUMATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Traditionally rheumatoid arthritis (RA) trials classify patients as responders and non-responders; they ignore the potential range of treatment responses. Group Based Trajectory Models (GBTMs) provide a more refined approach. They identify patient subgroups with similar outcome trajectories. We used GBTMs to classify patients into subgroups of varying responses and explore factors associated with different responses to intensive treatment in a secondary analysis of intensive treatment in the TITRATE clinical trial.
Methods: The TITRATE trial enrolled 335 patients with RA: 168 patients were randomised to receive intensive management, which comprised monthly assessments including measures of the disease activity score for 28 joints (DAS28), treatment escalation when patients were not responding sufficiently and psychosocial support; 163 of these patients completed the trial. We applied GBTMs to monthly DAS28 scores over one year to these patients who had received intensive management. The control group had standard care and were assessed every 6 months; they had too few DAS28 scores for applying GBTMs.
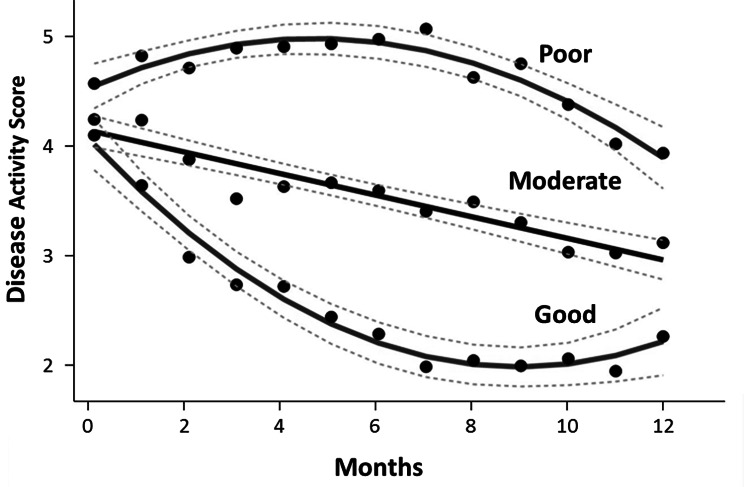
Results: GBTMs identified three distinct trajectories in the patients receiving intensive management: good (n = 40), moderate (n = 76) and poor (n = 47) responders. Baseline body mass index (BMI), disability, fatigue and depression levels were significantly different between trajectory groups. Few (10%) good responders were obese, compared to 38% of moderate, and 43% of poor responders (P = 0.002). Few (8%) good responders had depression, compared to 14% moderate responders, and 38% poor responders (P < 0.001). The key difference in treatments was using high-cost biologics, used in only 5% of good responders but 30% of moderate and 51% of poor responders (P < 0.001). Most good responders had endpoint remissions and low disability, pain, and fatigue scores; few poor responders achieved any favourable outcomes.
Conclusion: GBTMs identified three trajectories of disease activity progression in patients receiving intensive management for moderately active RA. Baseline variables like obesity and depression predicted different treatment responses. Few good responders needed biologic drugs; they responded to conventional DMARDs alone. GBTMs have the potential to facilitate precision medicine enabling patient-oriented treatment strategies based on key characteristics.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
