Risk of subsequent lower respiratory tract infection (LRTI) after hospitalization for COVID-19 LRTI and non-COVID-19 LRTI: a retrospective cohort study.
Katia J Bruxvoort, Heidi Fischer, Joseph A Lewnard, Vennis X Hong, Magdalena Pomichowski, Lindsay R Grant, Luis Jódar, Bradford D Gessner, Sara Y Tartof
{"title":"Risk of subsequent lower respiratory tract infection (LRTI) after hospitalization for COVID-19 LRTI and non-COVID-19 LRTI: a retrospective cohort study.","authors":"Katia J Bruxvoort, Heidi Fischer, Joseph A Lewnard, Vennis X Hong, Magdalena Pomichowski, Lindsay R Grant, Luis Jódar, Bradford D Gessner, Sara Y Tartof","doi":"10.1186/s41479-023-00117-5","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Respiratory pathogens, including SARS-CoV-2, can cause pulmonary structural damage and physiologic impairment, which may increase the risk of subsequent lower respiratory tract infections (LRTI). Prior hospitalization for any reason is a risk factor for LRTI, but data on the risk of subsequent new-onset LRTI following hospitalization for COVID-19 LRTI or non-COVID-19 LRTI are needed to inform strategies for immunizations targeting respiratory pathogens.</p><p><strong>Methods: </strong>We conducted a retrospective cohort study at Kaiser Permanente Southern California (KPSC) among adults hospitalized from 3/1/2020 to 5/31/2022, excluding labor and delivery. We categorized individuals into 3 mutually exclusive baseline exposure groups: those hospitalized for COVID-19 LRTI, those hospitalized for non-COVID-19 LRTI, and those hospitalized for all other causes without LRTI or COVID-19 (\"non-LRTI\"). Following hospital discharge, patients were followed up for new-onset LRTI, beginning 30 antibiotic-free days after hospital discharge until 8/31/2022. We used multivariable cause-specific Cox regression with time-varying covariates to estimate hazard ratios (HR) of new-onset LRTI comparing those hospitalized for COVID-19 LRTI or non-COVID-19 LRTI to those hospitalized for non-LRTI, adjusting for demographic and clinical characteristics.</p><p><strong>Results: </strong>The study included 22,417 individuals hospitalized for COVID-19 LRTI, 12,795 individuals hospitalized for non-COVID-19 LRTI, and 176,788 individuals hospitalized for non-LRTI. Individuals hospitalized for non-COVID-19 LRTI were older and had more comorbidities than those hospitalized for COVID-19 LRTI or non-LRTI. Incidence rates per 1,000 person-years (95% CI) of new-onset LRTI were 52.5 (51.4-53.6) among individuals hospitalized for COVID-19 LRTI, 253.5 (243.7-263.6) among those hospitalized for non-COVID-19 LRTI, and 52.5 (51.4-53.6) among those hospitalized for non-LRTI. The adjusted hazard of new-onset LRTI during follow-up was 20% higher among individuals hospitalized for COVID-19 LRTI (HR 1.20 [95% CI: 1.12-1.28]) and 301% higher among individuals hospitalized for non-COVID-19 LRTI (HR 3.01 [95% CI: 2.87-3.15]) compared to those hospitalized for non-LRTI.</p><p><strong>Conclusion: </strong>The risk of new-onset LRTI following hospital discharge was high, particularly among those hospitalized for non-COVID-19 LRTI, but also for COVID-19 LRTI. These data suggest that immunizations targeting respiratory pathogens, including COVID-19, should be considered for adults hospitalized for LRTI prior to hospital discharge.</p>","PeriodicalId":45120,"journal":{"name":"Pneumonia","volume":"15 1","pages":"15"},"PeriodicalIF":6.2000,"publicationDate":"2023-10-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10552217/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pneumonia","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s41479-023-00117-5","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"RESPIRATORY SYSTEM","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Respiratory pathogens, including SARS-CoV-2, can cause pulmonary structural damage and physiologic impairment, which may increase the risk of subsequent lower respiratory tract infections (LRTI). Prior hospitalization for any reason is a risk factor for LRTI, but data on the risk of subsequent new-onset LRTI following hospitalization for COVID-19 LRTI or non-COVID-19 LRTI are needed to inform strategies for immunizations targeting respiratory pathogens.
Methods: We conducted a retrospective cohort study at Kaiser Permanente Southern California (KPSC) among adults hospitalized from 3/1/2020 to 5/31/2022, excluding labor and delivery. We categorized individuals into 3 mutually exclusive baseline exposure groups: those hospitalized for COVID-19 LRTI, those hospitalized for non-COVID-19 LRTI, and those hospitalized for all other causes without LRTI or COVID-19 ("non-LRTI"). Following hospital discharge, patients were followed up for new-onset LRTI, beginning 30 antibiotic-free days after hospital discharge until 8/31/2022. We used multivariable cause-specific Cox regression with time-varying covariates to estimate hazard ratios (HR) of new-onset LRTI comparing those hospitalized for COVID-19 LRTI or non-COVID-19 LRTI to those hospitalized for non-LRTI, adjusting for demographic and clinical characteristics.
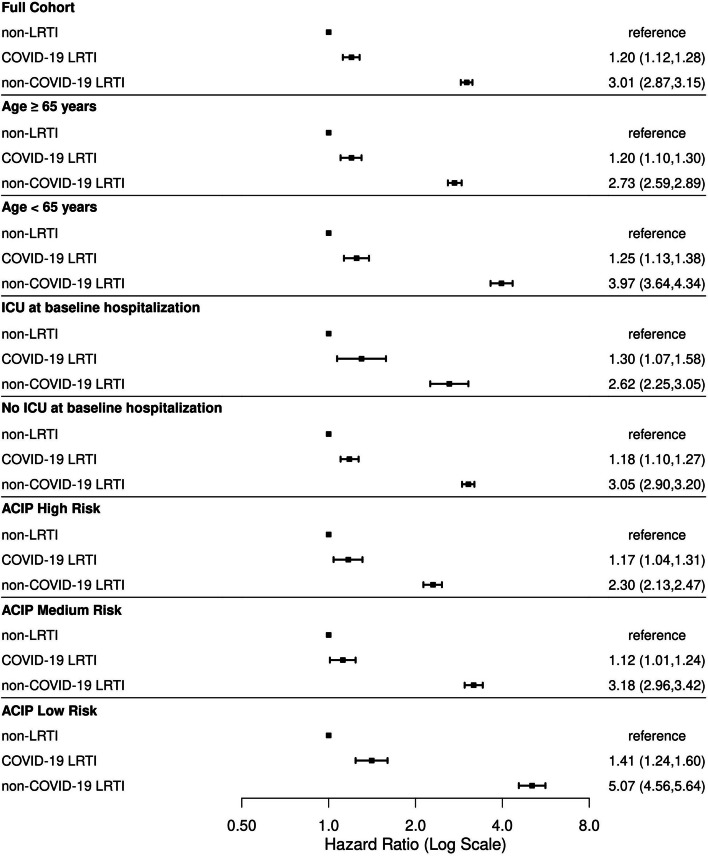
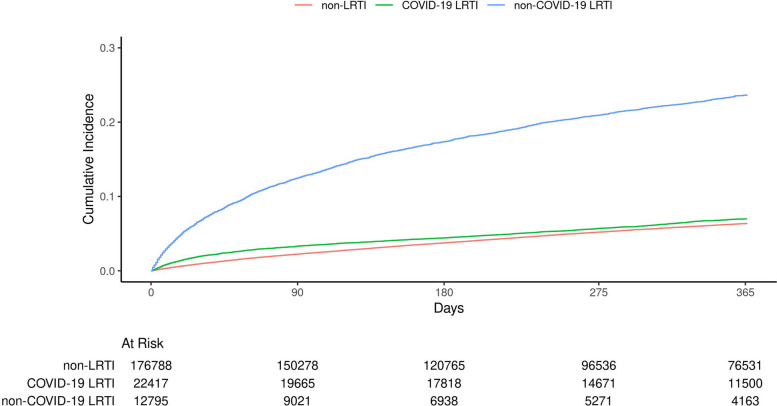
Results: The study included 22,417 individuals hospitalized for COVID-19 LRTI, 12,795 individuals hospitalized for non-COVID-19 LRTI, and 176,788 individuals hospitalized for non-LRTI. Individuals hospitalized for non-COVID-19 LRTI were older and had more comorbidities than those hospitalized for COVID-19 LRTI or non-LRTI. Incidence rates per 1,000 person-years (95% CI) of new-onset LRTI were 52.5 (51.4-53.6) among individuals hospitalized for COVID-19 LRTI, 253.5 (243.7-263.6) among those hospitalized for non-COVID-19 LRTI, and 52.5 (51.4-53.6) among those hospitalized for non-LRTI. The adjusted hazard of new-onset LRTI during follow-up was 20% higher among individuals hospitalized for COVID-19 LRTI (HR 1.20 [95% CI: 1.12-1.28]) and 301% higher among individuals hospitalized for non-COVID-19 LRTI (HR 3.01 [95% CI: 2.87-3.15]) compared to those hospitalized for non-LRTI.
Conclusion: The risk of new-onset LRTI following hospital discharge was high, particularly among those hospitalized for non-COVID-19 LRTI, but also for COVID-19 LRTI. These data suggest that immunizations targeting respiratory pathogens, including COVID-19, should be considered for adults hospitalized for LRTI prior to hospital discharge.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
