Optimizing the Equitable Deployment of Virtual Care for Women: Protocol for a Qualitative Evidence Synthesis Examining Patient and Provider Perspectives Supplemented with Primary Qualitative Data.
Karen M Goldstein, Dhara B Patel, Katherine A Van Loon, Abigail Shapiro, Sharron Rushton, Allison A Lewinski, Tiera J Lanford, Sarah Cantrell, Leah L Zullig, Sarah M Wilson, Megan Shepherd-Banigan, Susan Alton Dailey, Catherine Sims, Cheryl Robinson, Neetu Chawla, Hayden B Bosworth, Alison Hamilton, Jennifer Naylor, Jennifer M Gierisch
{"title":"Optimizing the Equitable Deployment of Virtual Care for Women: Protocol for a Qualitative Evidence Synthesis Examining Patient and Provider Perspectives Supplemented with Primary Qualitative Data.","authors":"Karen M Goldstein, Dhara B Patel, Katherine A Van Loon, Abigail Shapiro, Sharron Rushton, Allison A Lewinski, Tiera J Lanford, Sarah Cantrell, Leah L Zullig, Sarah M Wilson, Megan Shepherd-Banigan, Susan Alton Dailey, Catherine Sims, Cheryl Robinson, Neetu Chawla, Hayden B Bosworth, Alison Hamilton, Jennifer Naylor, Jennifer M Gierisch","doi":"10.1089/heq.2023.0089","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Women experience numerous barriers to patient-centered health care (e.g., lack of continuity). Such barriers are amplified for women from marginalized communities. Virtual care may improve equitable access. We are conducting a partner-engaged, qualitative evidence synthesis (QES) of patients' and providers' experiences with virtual health care delivery for women.</p><p><strong>Methods: </strong>We use a best-fit framework approach informed by the Non-adoption, Abandonment, Scale-up, Spread, and Sustainability framework and Public Health Critical Race Praxis. We will supplement published literature with qualitative interviews with women from underrepresented communities and their health care providers. We will engage patients and other contributors through multiple participatory methods.</p><p><strong>Results: </strong>Our search identified 5525 articles published from 2010 to 2022. Sixty were eligible, of which 42 focused on women and 24 on provider experiences. Data abstraction and analysis are ongoing.</p><p><strong>Discussion: </strong>This work offers four key innovations to advance health equity: (1) conceptual foundation rooted in an antiracist action-oriented praxis; (2) worked example of centering QES on marginalized communities; (3) supplementing QES with primary qualitative information with populations historically marginalized in the health care system; and (4) participatory approaches that foster longitudinal partnered engagement.</p><p><strong>Health equity implications: </strong>Our approach to exploring virtual health care for women demonstrates an antiracist praxis to inform knowledge generation. In doing so, we aim to generate findings that can guide health care systems in the equitable deployment of comprehensive virtual care for women.</p>","PeriodicalId":36602,"journal":{"name":"Health Equity","volume":"7 1","pages":"570-580"},"PeriodicalIF":2.5000,"publicationDate":"2023-09-13","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10507937/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Health Equity","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1089/heq.2023.0089","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"PUBLIC, ENVIRONMENTAL & OCCUPATIONAL HEALTH","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Women experience numerous barriers to patient-centered health care (e.g., lack of continuity). Such barriers are amplified for women from marginalized communities. Virtual care may improve equitable access. We are conducting a partner-engaged, qualitative evidence synthesis (QES) of patients' and providers' experiences with virtual health care delivery for women.
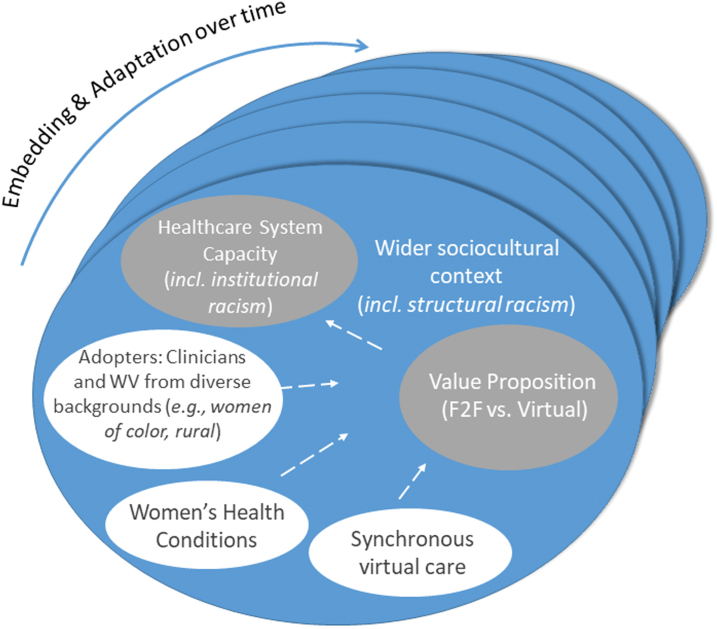
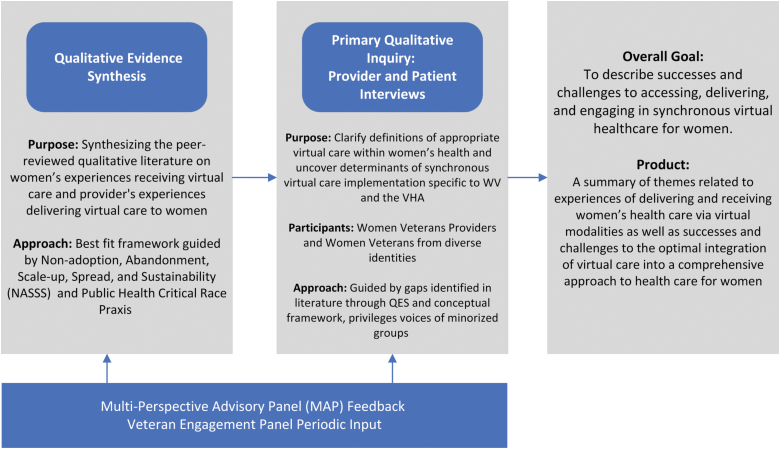
Methods: We use a best-fit framework approach informed by the Non-adoption, Abandonment, Scale-up, Spread, and Sustainability framework and Public Health Critical Race Praxis. We will supplement published literature with qualitative interviews with women from underrepresented communities and their health care providers. We will engage patients and other contributors through multiple participatory methods.
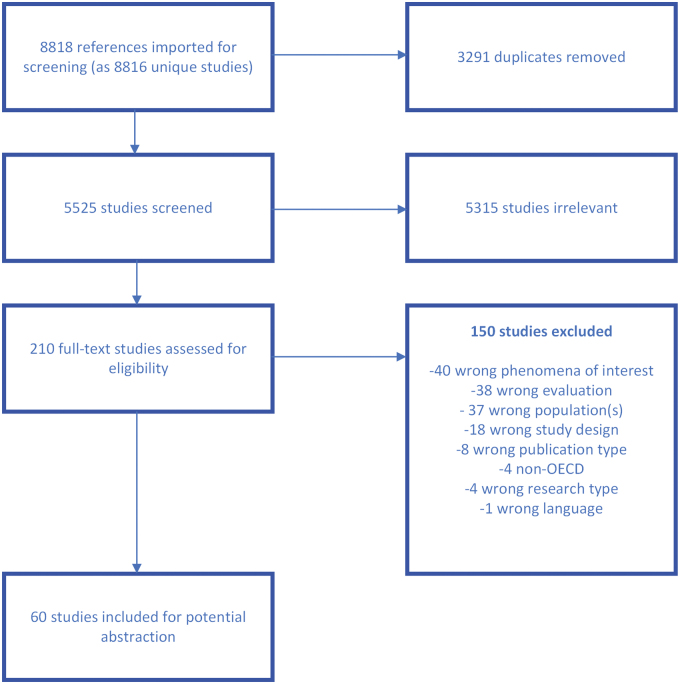
Results: Our search identified 5525 articles published from 2010 to 2022. Sixty were eligible, of which 42 focused on women and 24 on provider experiences. Data abstraction and analysis are ongoing.
Discussion: This work offers four key innovations to advance health equity: (1) conceptual foundation rooted in an antiracist action-oriented praxis; (2) worked example of centering QES on marginalized communities; (3) supplementing QES with primary qualitative information with populations historically marginalized in the health care system; and (4) participatory approaches that foster longitudinal partnered engagement.
Health equity implications: Our approach to exploring virtual health care for women demonstrates an antiracist praxis to inform knowledge generation. In doing so, we aim to generate findings that can guide health care systems in the equitable deployment of comprehensive virtual care for women.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
