Jennifer Mallow, Stephen M Davis, Johnathan Herczyk, Margaret Jaynes, Ben Klos, Marcus Canaday, Laurie Theeke
{"title":"Feasibility and Acceptability of Community-Based Telehealth to Prevent Long-Term Care Readmission.","authors":"Jennifer Mallow, Stephen M Davis, Johnathan Herczyk, Margaret Jaynes, Ben Klos, Marcus Canaday, Laurie Theeke","doi":"10.1089/tmr.2022.0040","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Transitioning to community living after long-term care requires multiple complex individualized interventions to prevent readmission. The current focus of home and community-based services (HCBS) is on increasing consumer engagement and individualizing care. Telehealth interventions provide additional services without the burden of face-to-face encounters and have yet to be evaluated for feasibility and acceptability in rural HCBS.</p><p><strong>Methods: </strong>West Virginia Bureau for Medical Services and West Virginia University implemented and evaluated a telehealth intervention with 26 Aged and Disabled Waiver or Traumatic Brain Injury Waiver participants who were transitioning back into their communities from a long-term care facility. Feasibility was assessed through recruitment process, fidelity to planned intervention, number of people eligible for participation, number of individuals enrolling in the intervention, enrollment process, completed enrollment, engagement in the intervention, number of weeks participating in the intervention, type of devices provided, attrition, and fidelity to original intervention. Satisfaction with services was used as a marker of acceptability for both participants and providers.</p><p><strong>Results: </strong>Half (<i>n</i> = 12) of the enrolled population completed the full 24-week telehealth monitoring period and modification of the original intervention was necessary for most. Provider and participant satisfaction was high. Recruitment and enrollment may have been affected by COVID-19.</p><p><strong>Conclusion: </strong>Future implementation will continue to track recruitment and retention efforts. Individualized care plans, demonstration and practice with equipment, family or direct-care worker presence, and live technical support through the phone are needed. Primary care provider and in-home direct-care worker satisfaction workflow planning and evaluation are required.</p>","PeriodicalId":94218,"journal":{"name":"Telemedicine reports","volume":"4 1","pages":"135-146"},"PeriodicalIF":1.6000,"publicationDate":"2023-06-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10523410/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Telemedicine reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1089/tmr.2022.0040","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Transitioning to community living after long-term care requires multiple complex individualized interventions to prevent readmission. The current focus of home and community-based services (HCBS) is on increasing consumer engagement and individualizing care. Telehealth interventions provide additional services without the burden of face-to-face encounters and have yet to be evaluated for feasibility and acceptability in rural HCBS.
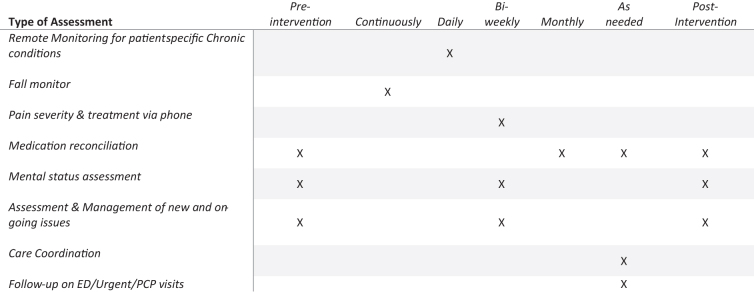
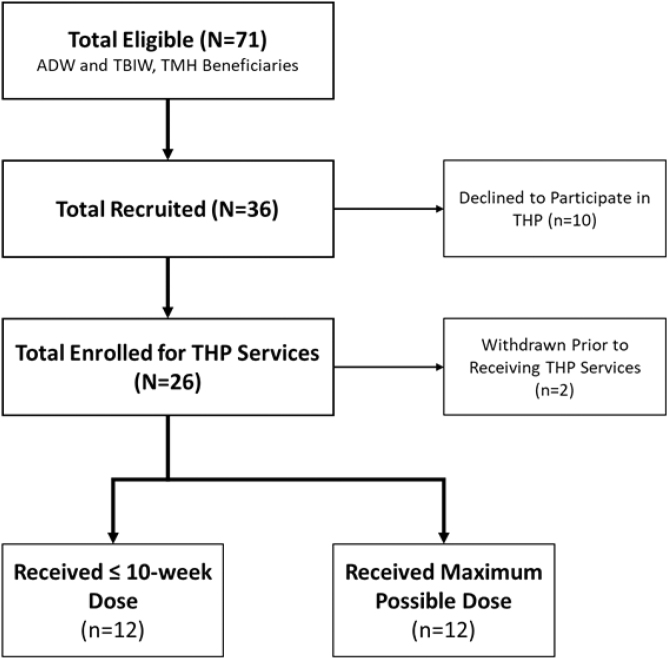
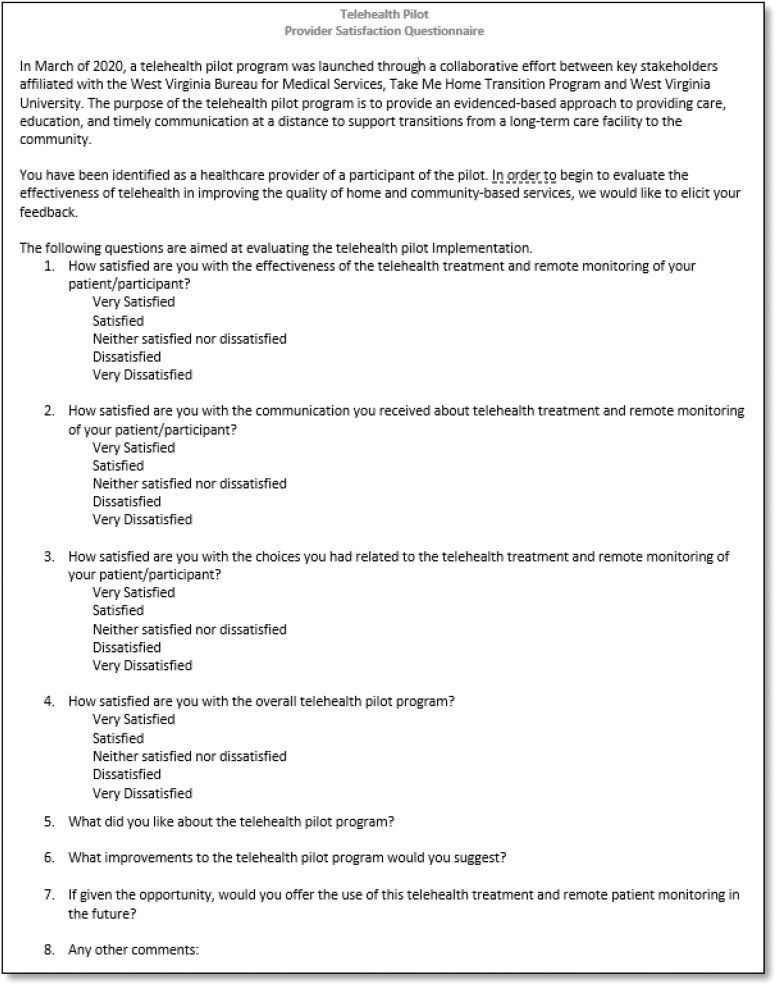
Methods: West Virginia Bureau for Medical Services and West Virginia University implemented and evaluated a telehealth intervention with 26 Aged and Disabled Waiver or Traumatic Brain Injury Waiver participants who were transitioning back into their communities from a long-term care facility. Feasibility was assessed through recruitment process, fidelity to planned intervention, number of people eligible for participation, number of individuals enrolling in the intervention, enrollment process, completed enrollment, engagement in the intervention, number of weeks participating in the intervention, type of devices provided, attrition, and fidelity to original intervention. Satisfaction with services was used as a marker of acceptability for both participants and providers.
Results: Half (n = 12) of the enrolled population completed the full 24-week telehealth monitoring period and modification of the original intervention was necessary for most. Provider and participant satisfaction was high. Recruitment and enrollment may have been affected by COVID-19.
Conclusion: Future implementation will continue to track recruitment and retention efforts. Individualized care plans, demonstration and practice with equipment, family or direct-care worker presence, and live technical support through the phone are needed. Primary care provider and in-home direct-care worker satisfaction workflow planning and evaluation are required.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
