Pierluigi Fusco, Angela Iuorio, Mirco Della Valle, Fausto Ferraro
{"title":"Awake tracheostomy in a patient with acute upper airway obstruction: an emergency application of an elective percutaneous procedure.","authors":"Pierluigi Fusco, Angela Iuorio, Mirco Della Valle, Fausto Ferraro","doi":"10.2147/OAEM.S201079","DOIUrl":null,"url":null,"abstract":"<p><p>Since its introduction in 1985 with Ciaglia, percutaneous tracheostomy (PT) was contraindicated in emergency settings and obesity. However, several case series in the last 20 years have documented the use of PT in life-threatening airway emergencies. We present a case of severe acute airway obstruction in a 66-year-old woman successfully treated with a placement of an awake PT. The woman's glottic obstruction was caused by a recurrent laryngeal neoplasia and revealed by nasoendoscopy. This acute condition required a serious effort from the patient to oxygenate and therefore prevented orotracheal intubation as well as the use of any supraglottic device and/or sedation. Blood aspiration after a first attempt to make a quick access to the tracheal lumen with an emergency cricothyroidotomy, and difficulties in the exact identification of tumor infiltration, led us to perform an awake tracheostomy. Due to elevated risk of airway bleeding, we started with a surgical approach to better identify anatomical structures. After the correct inter-tracheal ring space identification, sudden worsening of clinical symptoms required that we complete the procedure quickly with the aid of a Ciaglia Blue Rhino™-Cook (CBR) tracheostomy kit. At the tracheostomy tube placement, the patient quickly resolved her dyspnea and physiological breathing was restored.</p>","PeriodicalId":45096,"journal":{"name":"Open Access Emergency Medicine","volume":"11 ","pages":"167-170"},"PeriodicalIF":1.5000,"publicationDate":"2019-07-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/68/e2/oaem-11-167.PMC6661998.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Open Access Emergency Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/OAEM.S201079","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2019/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"EMERGENCY MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
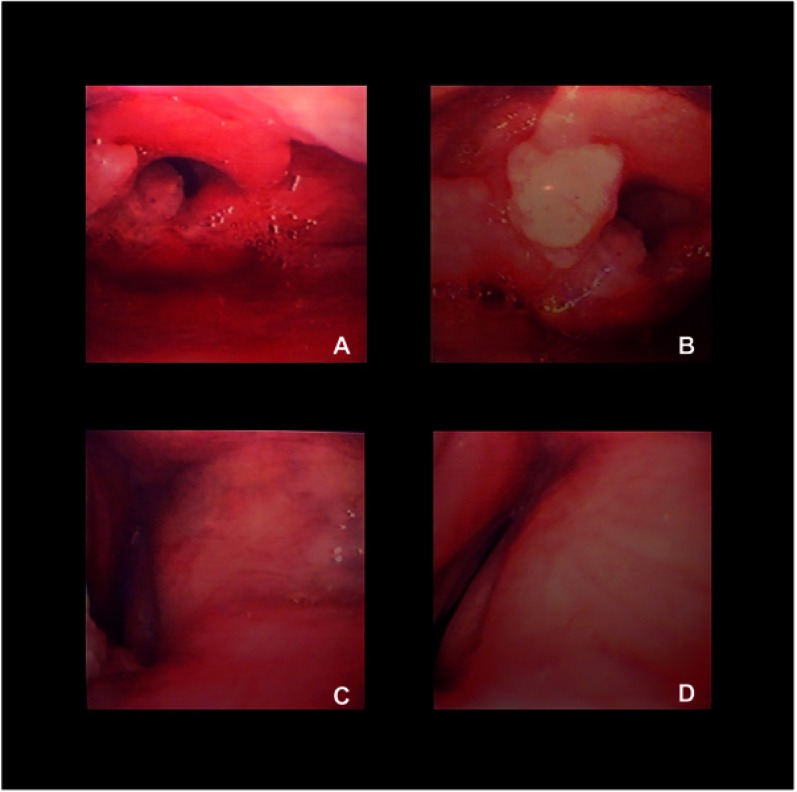
Since its introduction in 1985 with Ciaglia, percutaneous tracheostomy (PT) was contraindicated in emergency settings and obesity. However, several case series in the last 20 years have documented the use of PT in life-threatening airway emergencies. We present a case of severe acute airway obstruction in a 66-year-old woman successfully treated with a placement of an awake PT. The woman's glottic obstruction was caused by a recurrent laryngeal neoplasia and revealed by nasoendoscopy. This acute condition required a serious effort from the patient to oxygenate and therefore prevented orotracheal intubation as well as the use of any supraglottic device and/or sedation. Blood aspiration after a first attempt to make a quick access to the tracheal lumen with an emergency cricothyroidotomy, and difficulties in the exact identification of tumor infiltration, led us to perform an awake tracheostomy. Due to elevated risk of airway bleeding, we started with a surgical approach to better identify anatomical structures. After the correct inter-tracheal ring space identification, sudden worsening of clinical symptoms required that we complete the procedure quickly with the aid of a Ciaglia Blue Rhino™-Cook (CBR) tracheostomy kit. At the tracheostomy tube placement, the patient quickly resolved her dyspnea and physiological breathing was restored.
自1985年Ciaglia问世以来,经皮气管造口术(PT)在急诊和肥胖中是禁忌。然而,在过去20年中的几个案例系列已经记录了PT在危及生命的气道紧急情况中的使用。我们报告了一例66岁女性的严重急性气道阻塞,成功地放置了清醒的PT。该女性的声门阻塞是由复发性喉肿瘤引起的,并通过鼻内镜检查显示。这种急性情况需要患者认真努力给氧,因此阻止了经口气管插管以及使用任何声门上装置和/或镇静。在第一次尝试用紧急环甲切开术快速进入气管腔后进行抽血,并且难以准确识别肿瘤浸润,导致我们进行了清醒的气管造口术。由于气道出血的风险增加,我们从手术方法开始,以更好地识别解剖结构。在正确识别气管环间隙后,临床症状的突然恶化需要我们在Ciaglia Blue Rhino的帮助下快速完成手术™-Cook(CBR)气管造口试剂盒。气管切开插管时,患者的呼吸困难很快得到缓解,生理呼吸得以恢复。



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
