Comparing antibiotic prescribing between clinicians in UK primary care: an analysis in a cohort study of eight different measures of antibiotic prescribing.
Tjeerd Van Staa, Yan Li, Natalie Gold, Tim Chadborn, William Welfare, Victoria Palin, Darren M Ashcroft, Joanna Bircher
{"title":"Comparing antibiotic prescribing between clinicians in UK primary care: an analysis in a cohort study of eight different measures of antibiotic prescribing.","authors":"Tjeerd Van Staa, Yan Li, Natalie Gold, Tim Chadborn, William Welfare, Victoria Palin, Darren M Ashcroft, Joanna Bircher","doi":"10.1136/bmjqs-2020-012108","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>There is a need to reduce antimicrobial uses in humans. Previous studies have found variations in antibiotic (AB) prescribing between practices in primary care. This study assessed variability of AB prescribing between clinicians.</p><p><strong>Methods: </strong>Clinical Practice Research Datalink, which collects electronic health records in primary care, was used to select anonymised clinicians providing 500+ consultations during 2012-2017. Eight measures of AB prescribing were assessed, such as overall and incidental AB prescribing, repeat AB courses and extent of risk-based prescribing. Poisson regression models with random effect for clinicians were fitted.</p><p><strong>Results: </strong>6111 clinicians from 466 general practices were included. Considerable variability between individual clinicians was found for most AB measures. For example, the rate of AB prescribing varied between 77.4 and 350.3 per 1000 consultations; percentage of repeat AB courses within 30 days ranged from 13.1% to 34.3%; predicted patient risk of hospital admission for infection-related complications in those prescribed AB ranged from 0.03% to 0.32% (5th and 95th percentiles). The adjusted relative rate between clinicians in rates of AB prescribing was 5.23. Weak correlation coefficients (<0.5) were found between most AB measures. There was considerable variability in case mix seen by clinicians. The largest potential impact to reduce AB prescribing could be around encouraging risk-based prescribing and addressing repeat issues of ABs. Reduction of repeat AB courses to prescribing habit of median clinician would save 21 813 AB prescriptions per 1000 clinicians per year.</p><p><strong>Conclusions: </strong>The wide variation seen in all measures of AB prescribing and weak correlation between them suggests that a single AB measure, such as prescribing rate, is not sufficient to underpin the optimisation of AB prescribing.</p>","PeriodicalId":49653,"journal":{"name":"Quality & Safety in Health Care","volume":"31 1","pages":"831-838"},"PeriodicalIF":0.0000,"publicationDate":"2022-10-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9606525/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Quality & Safety in Health Care","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1136/bmjqs-2020-012108","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: There is a need to reduce antimicrobial uses in humans. Previous studies have found variations in antibiotic (AB) prescribing between practices in primary care. This study assessed variability of AB prescribing between clinicians.
Methods: Clinical Practice Research Datalink, which collects electronic health records in primary care, was used to select anonymised clinicians providing 500+ consultations during 2012-2017. Eight measures of AB prescribing were assessed, such as overall and incidental AB prescribing, repeat AB courses and extent of risk-based prescribing. Poisson regression models with random effect for clinicians were fitted.
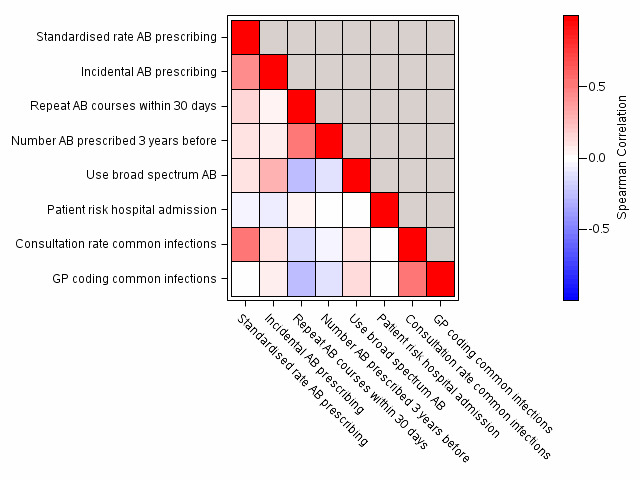
Results: 6111 clinicians from 466 general practices were included. Considerable variability between individual clinicians was found for most AB measures. For example, the rate of AB prescribing varied between 77.4 and 350.3 per 1000 consultations; percentage of repeat AB courses within 30 days ranged from 13.1% to 34.3%; predicted patient risk of hospital admission for infection-related complications in those prescribed AB ranged from 0.03% to 0.32% (5th and 95th percentiles). The adjusted relative rate between clinicians in rates of AB prescribing was 5.23. Weak correlation coefficients (<0.5) were found between most AB measures. There was considerable variability in case mix seen by clinicians. The largest potential impact to reduce AB prescribing could be around encouraging risk-based prescribing and addressing repeat issues of ABs. Reduction of repeat AB courses to prescribing habit of median clinician would save 21 813 AB prescriptions per 1000 clinicians per year.
Conclusions: The wide variation seen in all measures of AB prescribing and weak correlation between them suggests that a single AB measure, such as prescribing rate, is not sufficient to underpin the optimisation of AB prescribing.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
