Carl Marincowitz, Tony Stone, Peter Bath, Richard Campbell, Janette Kay Turner, Madina Hasan, Richard Pilbery, Benjamin David Thomas, Laura Sutton, Fiona Bell, Katie Biggs, Frank Hopfgartner, Suvodeep Mazumdar, Jennifer Petrie, Steve Goodacre
{"title":"Accuracy of telephone triage for predicting adverse outcomes in suspected COVID-19: an observational cohort study.","authors":"Carl Marincowitz, Tony Stone, Peter Bath, Richard Campbell, Janette Kay Turner, Madina Hasan, Richard Pilbery, Benjamin David Thomas, Laura Sutton, Fiona Bell, Katie Biggs, Frank Hopfgartner, Suvodeep Mazumdar, Jennifer Petrie, Steve Goodacre","doi":"10.1136/bmjqs-2021-014382","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>To assess accuracy of telephone triage in identifying need for emergency care among those with suspected COVID-19 infection and identify factors which affect triage accuracy.</p><p><strong>Design: </strong>Observational cohort study.</p><p><strong>Setting: </strong>Community telephone triage provided in the UK by Yorkshire Ambulance Service NHS Trust (YAS).</p><p><strong>Participants: </strong>40 261 adults who contacted National Health Service (NHS) 111 telephone triage services provided by YAS between 18 March 2020 and 29 June 2020 with symptoms indicating COVID-19 infection were linked to Office for National Statistics death registrations and healthcare data collected by NHS Digital.</p><p><strong>Outcome: </strong>Accuracy of triage disposition was assessed in terms of death or need for organ support up to 30 days from first contact.</p><p><strong>Results: </strong>Callers had a 3% (1200/40 261) risk of serious adverse outcomes (death or organ support). Telephone triage recommended self-care or non-urgent assessment for 60% (24 335/40 261), with a 1.3% (310/24 335) risk of adverse outcomes. Telephone triage had 74.2% sensitivity (95% CI: 71.6 to 76.6%) and 61.5% specificity (95% CI: 61% to 62%) for the primary outcome. Multivariable analysis suggested respiratory comorbidities may be overappreciated, and diabetes underappreciated as predictors of deterioration. Repeat contact with triage service appears to be an important under-recognised predictor of deterioration with 2 contacts (OR 1.77, 95% CI: 1.14 to 2.75) and 3 or more contacts (OR 4.02, 95% CI: 1.68 to 9.65) associated with false negative triage.</p><p><strong>Conclusion: </strong>Patients advised to self-care or receive non-urgent clinical assessment had a small but non-negligible risk of serious clinical deterioration. Repeat contact with telephone services needs recognition as an important predictor of subsequent adverse outcomes.</p>","PeriodicalId":49653,"journal":{"name":"Quality & Safety in Health Care","volume":"1 1","pages":"375-385"},"PeriodicalIF":0.0000,"publicationDate":"2024-05-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8983415/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Quality & Safety in Health Care","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1136/bmjqs-2021-014382","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: To assess accuracy of telephone triage in identifying need for emergency care among those with suspected COVID-19 infection and identify factors which affect triage accuracy.
Design: Observational cohort study.
Setting: Community telephone triage provided in the UK by Yorkshire Ambulance Service NHS Trust (YAS).
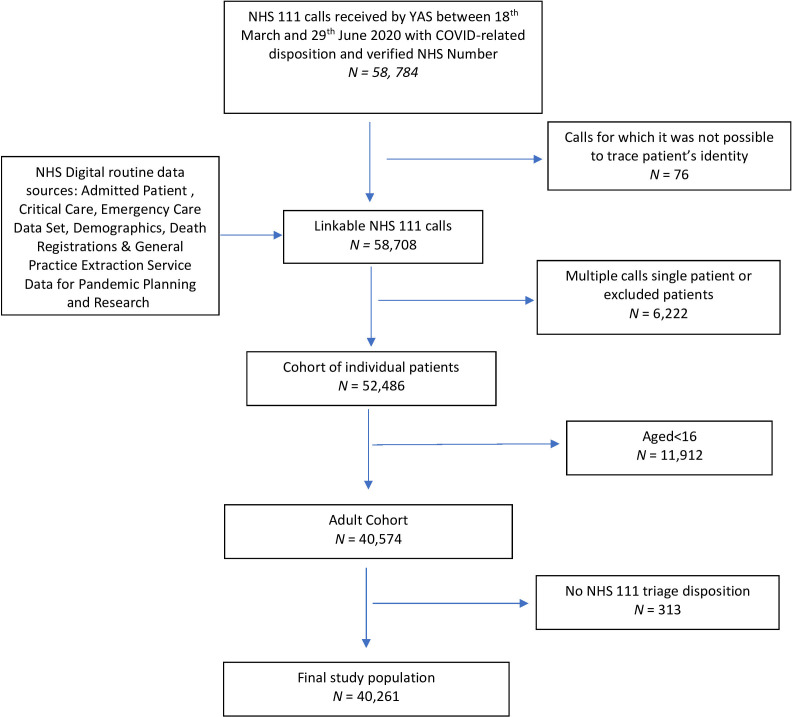
Participants: 40 261 adults who contacted National Health Service (NHS) 111 telephone triage services provided by YAS between 18 March 2020 and 29 June 2020 with symptoms indicating COVID-19 infection were linked to Office for National Statistics death registrations and healthcare data collected by NHS Digital.
Outcome: Accuracy of triage disposition was assessed in terms of death or need for organ support up to 30 days from first contact.
Results: Callers had a 3% (1200/40 261) risk of serious adverse outcomes (death or organ support). Telephone triage recommended self-care or non-urgent assessment for 60% (24 335/40 261), with a 1.3% (310/24 335) risk of adverse outcomes. Telephone triage had 74.2% sensitivity (95% CI: 71.6 to 76.6%) and 61.5% specificity (95% CI: 61% to 62%) for the primary outcome. Multivariable analysis suggested respiratory comorbidities may be overappreciated, and diabetes underappreciated as predictors of deterioration. Repeat contact with triage service appears to be an important under-recognised predictor of deterioration with 2 contacts (OR 1.77, 95% CI: 1.14 to 2.75) and 3 or more contacts (OR 4.02, 95% CI: 1.68 to 9.65) associated with false negative triage.
Conclusion: Patients advised to self-care or receive non-urgent clinical assessment had a small but non-negligible risk of serious clinical deterioration. Repeat contact with telephone services needs recognition as an important predictor of subsequent adverse outcomes.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
