Can we identify the prevalence of perinatal mental health using routinely collected health data?: A review of publicly available perinatal mental health data sources in England
Sarah Masefield, Kathryn Willan, Zoe Darwin, Sarah Blower, Chandani Nekitsing, Josie Dickerson
{"title":"Can we identify the prevalence of perinatal mental health using routinely collected health data?: A review of publicly available perinatal mental health data sources in England","authors":"Sarah Masefield, Kathryn Willan, Zoe Darwin, Sarah Blower, Chandani Nekitsing, Josie Dickerson","doi":"10.1002/lrh2.10374","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Introduction</h3>\n \n <p>Perinatal mental health (PMH) conditions affect around one in four women, and may be even higher in women from some ethnic minority groups and those living in low socioeconomic circumstances. Poor PMH causes significant distress and can have lifelong adverse impacts for some children. In England, current prevalence rates are estimated using mental health data of the general population and do not take sociodemographic variance of geographical areas into account. Services cannot plan their capacity and ensure appropriate and timely support using these estimates. Our aim was to see if PMH prevalence rates could be identified using existing publicly available sources of routine health data.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>A review of data sources was completed by searching NHS Digital (now NHS England), Public Health England and other national PMH resources, performing keyword searches online, and research team knowledge of the field. The sources were screened for routine data that could be used to produce prevalence of PMH conditions by sociodemographic variation. Included sources were reviewed for their utility in accessibility, data relevance and technical specification relating to PMH and sociodemographic data items.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>We found a PMH data ‘blind spot’ with significant inadequacies in the utility of all identified data sources, making it impossible to provide information on the prevalence of PMH in England and understand variation by sociodemographic differences.</p>\n </section>\n \n <section>\n \n <h3> Conclusions</h3>\n \n <p>To enhance the utility of publicly available routine data to provide PMH prevalence rates requires improved mandatory PMH data capture in universal services, available publicly via one platform and including assessment outcomes and sociodemographic data.</p>\n </section>\n </div>","PeriodicalId":43916,"journal":{"name":"Learning Health Systems","volume":"8 1","pages":""},"PeriodicalIF":2.6000,"publicationDate":"2023-06-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/lrh2.10374","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Learning Health Systems","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/lrh2.10374","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"HEALTH POLICY & SERVICES","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction
Perinatal mental health (PMH) conditions affect around one in four women, and may be even higher in women from some ethnic minority groups and those living in low socioeconomic circumstances. Poor PMH causes significant distress and can have lifelong adverse impacts for some children. In England, current prevalence rates are estimated using mental health data of the general population and do not take sociodemographic variance of geographical areas into account. Services cannot plan their capacity and ensure appropriate and timely support using these estimates. Our aim was to see if PMH prevalence rates could be identified using existing publicly available sources of routine health data.
Methods
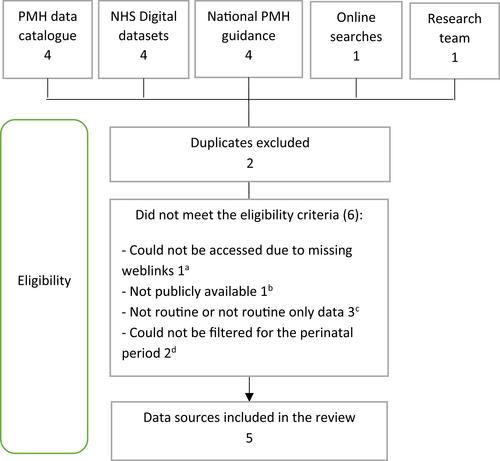
A review of data sources was completed by searching NHS Digital (now NHS England), Public Health England and other national PMH resources, performing keyword searches online, and research team knowledge of the field. The sources were screened for routine data that could be used to produce prevalence of PMH conditions by sociodemographic variation. Included sources were reviewed for their utility in accessibility, data relevance and technical specification relating to PMH and sociodemographic data items.
Results
We found a PMH data ‘blind spot’ with significant inadequacies in the utility of all identified data sources, making it impossible to provide information on the prevalence of PMH in England and understand variation by sociodemographic differences.
Conclusions
To enhance the utility of publicly available routine data to provide PMH prevalence rates requires improved mandatory PMH data capture in universal services, available publicly via one platform and including assessment outcomes and sociodemographic data.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
