Biswadev Mitra, Cristina Roman, Bertha Wu, Carl Luckhoff, Diana Goubrial, Timothy Amos, Holly Bannon-Murphy, Ronald Huynh, Michael Dooley, De Villiers Smit, Peter A Cameron
{"title":"Restriction of oxycodone in the emergency department (ROXY-ED): A randomised controlled trial.","authors":"Biswadev Mitra, Cristina Roman, Bertha Wu, Carl Luckhoff, Diana Goubrial, Timothy Amos, Holly Bannon-Murphy, Ronald Huynh, Michael Dooley, De Villiers Smit, Peter A Cameron","doi":"10.1177/20494637231189031","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The prescription of opioids in emergency care has been associated with harm, including overdose and dependence. The aim of this trial was to assess restriction of access to oxycodone (ROXY), in combination with education and guideline modifications, versus education and guideline modifications alone (standard care) to reduce oxycodone administration in the Emergency Department (ED).</p><p><strong>Methods: </strong>An unblinded, active control, randomised controlled trial was conducted in an adult tertiary ED. Participants were patients aged 18-75 years who had analgesics administered in the ED. The primary intervention was ROXY, through removal of all oxycodone immediate release tablets from the ED imprest, with availability of a small supply after senior clinician approval. The intervention did not restrict prescription of discharge medications. The primary outcome measure was oxycodone administration rates. Secondary outcomes were administration rates of other analgesic medications, time to initial analgesics and oxycodone prescription on discharge.</p><p><strong>Results: </strong>There were 2258 patients eligible for analysis. Oxycodone was administered to 80 (6.1%) patients in the ROXY group and 221 (23.3%) patients in the standard care group (relative risk (RR) 0.26; 95% CI: 0.21 to 0.33; <i>p</i> < .001). Tapentadol was prescribed more frequently in the ROXY group (RR 2.17; 95% CI: 1.71-2.74), while there were no differences in prescription of other analgesic medications. On discharge, significantly fewer patients were prescribed oxycodone (RR 0.51; 95% CI: 0.39-0.66) and no differences were observed in prescription rates of other analgesic medications. There was no difference in time to first analgesic (HR 0.94; 95% CI: 0.86-1.02).</p><p><strong>Conclusions: </strong>Restricted access to oxycodone was superior to education and guideline modifications alone for reducing oxycodone use in the ED and reducing discharge prescriptions of oxycodone from the ED. The addition of simple restrictive interventions is recommended to enable rapid changes to clinician behaviour to reduce the potential harm associated with the prescribing of oxycodone in the ED.</p>","PeriodicalId":46585,"journal":{"name":"British Journal of Pain","volume":"17 1","pages":"491-500"},"PeriodicalIF":1.5000,"publicationDate":"2023-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10722107/pdf/","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"British Journal of Pain","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/20494637231189031","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/7/12 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 1
Abstract
Background: The prescription of opioids in emergency care has been associated with harm, including overdose and dependence. The aim of this trial was to assess restriction of access to oxycodone (ROXY), in combination with education and guideline modifications, versus education and guideline modifications alone (standard care) to reduce oxycodone administration in the Emergency Department (ED).
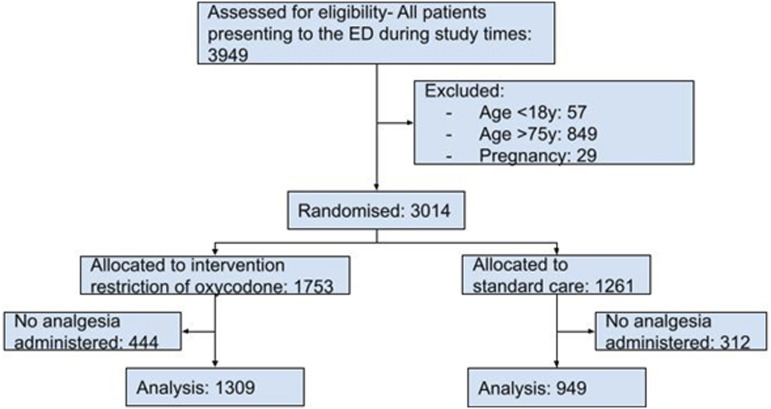
Methods: An unblinded, active control, randomised controlled trial was conducted in an adult tertiary ED. Participants were patients aged 18-75 years who had analgesics administered in the ED. The primary intervention was ROXY, through removal of all oxycodone immediate release tablets from the ED imprest, with availability of a small supply after senior clinician approval. The intervention did not restrict prescription of discharge medications. The primary outcome measure was oxycodone administration rates. Secondary outcomes were administration rates of other analgesic medications, time to initial analgesics and oxycodone prescription on discharge.
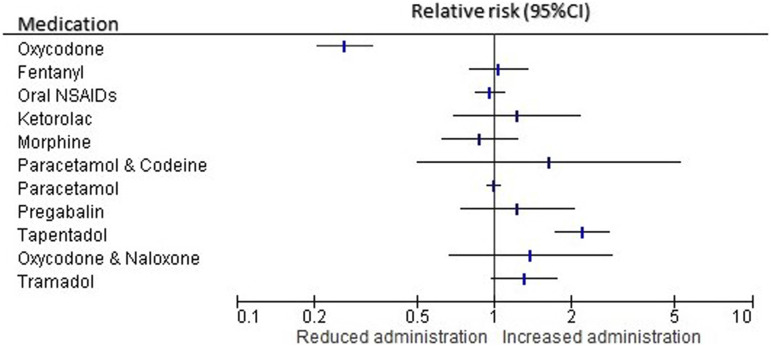
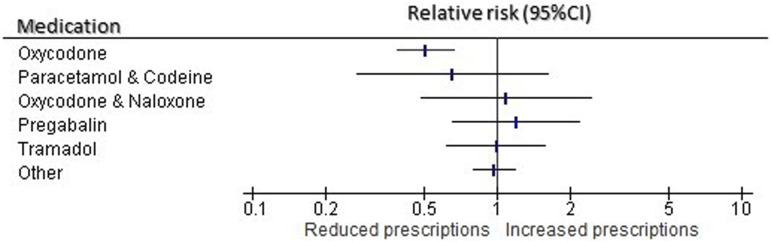
Results: There were 2258 patients eligible for analysis. Oxycodone was administered to 80 (6.1%) patients in the ROXY group and 221 (23.3%) patients in the standard care group (relative risk (RR) 0.26; 95% CI: 0.21 to 0.33; p < .001). Tapentadol was prescribed more frequently in the ROXY group (RR 2.17; 95% CI: 1.71-2.74), while there were no differences in prescription of other analgesic medications. On discharge, significantly fewer patients were prescribed oxycodone (RR 0.51; 95% CI: 0.39-0.66) and no differences were observed in prescription rates of other analgesic medications. There was no difference in time to first analgesic (HR 0.94; 95% CI: 0.86-1.02).
Conclusions: Restricted access to oxycodone was superior to education and guideline modifications alone for reducing oxycodone use in the ED and reducing discharge prescriptions of oxycodone from the ED. The addition of simple restrictive interventions is recommended to enable rapid changes to clinician behaviour to reduce the potential harm associated with the prescribing of oxycodone in the ED.
期刊介绍:
British Journal of Pain is a peer-reviewed quarterly British journal with an international multidisciplinary Editorial Board. The journal publishes original research and reviews on all major aspects of pain and pain management. Reviews reflect the body of evidence of the topic and are suitable for a multidisciplinary readership. Where empirical evidence is lacking, the reviews reflect the generally held opinions of experts in the field. The Journal has broadened its scope and has become a forum for publishing primary research together with brief reports related to pain and pain interventions. Submissions from all over the world have been published and are welcome. Official journal of the British Pain Society.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
