Mamas A Mamas, Marco Roffi, Ole Fröbert, Alaide Chieffo, Alessandro Beneduce, Andrija Matetic, Pim A L Tonino, Dragica Paunovic, Lotte Jacobs, Roxane Debrus, Jérémy El Aissaoui, Frank van Leeuwen, Evangelos Kontopantelis
{"title":"Predicting target lesion failure following percutaneous coronary intervention through machine learning risk assessment models.","authors":"Mamas A Mamas, Marco Roffi, Ole Fröbert, Alaide Chieffo, Alessandro Beneduce, Andrija Matetic, Pim A L Tonino, Dragica Paunovic, Lotte Jacobs, Roxane Debrus, Jérémy El Aissaoui, Frank van Leeuwen, Evangelos Kontopantelis","doi":"10.1093/ehjdh/ztad051","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>Central to the practice of precision medicine in percutaneous coronary intervention (PCI) is a risk-stratification tool to predict outcomes following the procedure. This study is intended to assess machine learning (ML)-based risk models to predict clinically relevant outcomes in PCI and to support individualized clinical decision-making in this setting.</p><p><strong>Methods and results: </strong>Five different ML models [gradient boosting classifier (GBC), linear discrimination analysis, Naïve Bayes, logistic regression, and K-nearest neighbours algorithm) for the prediction of 1-year target lesion failure (TLF) were trained on an extensive data set of 35 389 patients undergoing PCI and enrolled in the global, all-comers e-ULTIMASTER registry. The data set was split into a training (80%) and a test set (20%). Twenty-three patient and procedural characteristics were used as predictive variables. The models were compared for discrimination according to the area under the receiver operating characteristic curve (AUC) and for calibration. The GBC model showed the best discriminative ability with an AUC of 0.72 (95% confidence interval 0.69-0.75) for 1-year TLF on the test set. The discriminative ability of the GBC model for the components of TLF was highest for cardiac death with an AUC of 0.82, followed by target vessel myocardial infarction with an AUC of 0.75 and clinically driven target lesion revascularization with an AUC of 0.68. The calibration was fair until the highest risk deciles showed an underestimation of the risk.</p><p><strong>Conclusion: </strong>Machine learning-derived predictive models provide a reasonably accurate prediction of 1-year TLF in patients undergoing PCI. A prospective evaluation of the predictive score is warranted.</p><p><strong>Registration: </strong>Clinicaltrial.gov identifier is NCT02188355.</p>","PeriodicalId":3,"journal":{"name":"ACS Applied Electronic Materials","volume":" ","pages":"433-443"},"PeriodicalIF":4.7000,"publicationDate":"2023-08-31","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10689920/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"ACS Applied Electronic Materials","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/ehjdh/ztad051","RegionNum":3,"RegionCategory":"材料科学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/12/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"ENGINEERING, ELECTRICAL & ELECTRONIC","Score":null,"Total":0}
引用次数: 0
Abstract
Aims: Central to the practice of precision medicine in percutaneous coronary intervention (PCI) is a risk-stratification tool to predict outcomes following the procedure. This study is intended to assess machine learning (ML)-based risk models to predict clinically relevant outcomes in PCI and to support individualized clinical decision-making in this setting.
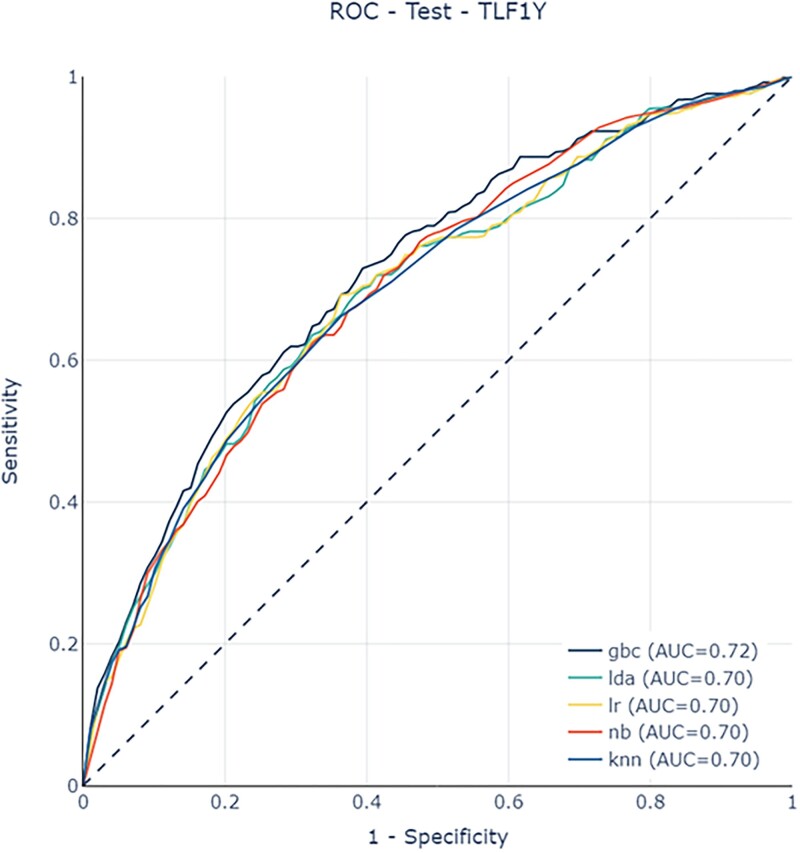
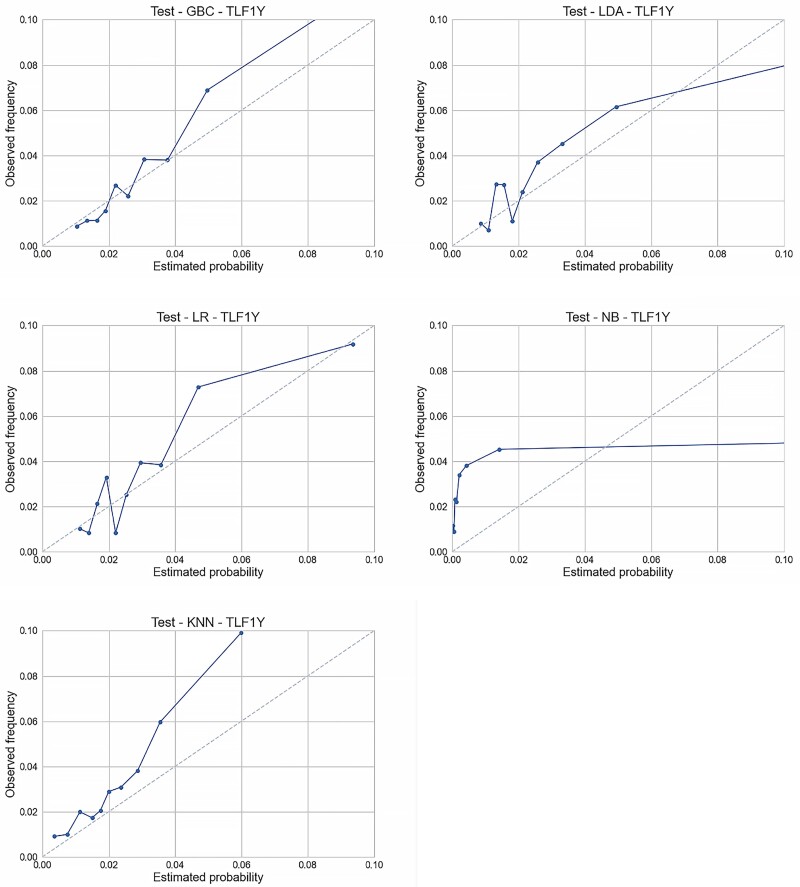
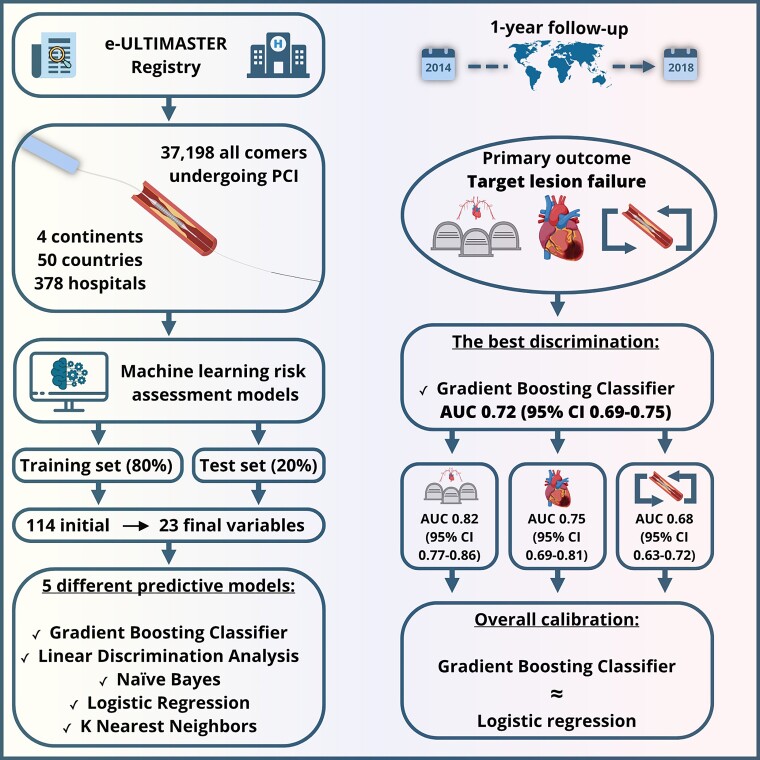
Methods and results: Five different ML models [gradient boosting classifier (GBC), linear discrimination analysis, Naïve Bayes, logistic regression, and K-nearest neighbours algorithm) for the prediction of 1-year target lesion failure (TLF) were trained on an extensive data set of 35 389 patients undergoing PCI and enrolled in the global, all-comers e-ULTIMASTER registry. The data set was split into a training (80%) and a test set (20%). Twenty-three patient and procedural characteristics were used as predictive variables. The models were compared for discrimination according to the area under the receiver operating characteristic curve (AUC) and for calibration. The GBC model showed the best discriminative ability with an AUC of 0.72 (95% confidence interval 0.69-0.75) for 1-year TLF on the test set. The discriminative ability of the GBC model for the components of TLF was highest for cardiac death with an AUC of 0.82, followed by target vessel myocardial infarction with an AUC of 0.75 and clinically driven target lesion revascularization with an AUC of 0.68. The calibration was fair until the highest risk deciles showed an underestimation of the risk.
Conclusion: Machine learning-derived predictive models provide a reasonably accurate prediction of 1-year TLF in patients undergoing PCI. A prospective evaluation of the predictive score is warranted.
Registration: Clinicaltrial.gov identifier is NCT02188355.
期刊介绍:
ACS Applied Electronic Materials is an interdisciplinary journal publishing original research covering all aspects of electronic materials. The journal is devoted to reports of new and original experimental and theoretical research of an applied nature that integrate knowledge in the areas of materials science, engineering, optics, physics, and chemistry into important applications of electronic materials. Sample research topics that span the journal's scope are inorganic, organic, ionic and polymeric materials with properties that include conducting, semiconducting, superconducting, insulating, dielectric, magnetic, optoelectronic, piezoelectric, ferroelectric and thermoelectric.
Indexed/Abstracted:
Web of Science SCIE
Scopus
CAS
INSPEC
Portico


 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
