Trend of sociodemographic and economic inequalities in the use of maternal health services in Lao People's Democratic Republic from 2006 to 2017: MICS data analysis.
Noudéhouénou Credo Adelphe Ahissou, Daisuke Nonaka, Rie Takeuchi, Calvin de Los Reyes, Manami Uehara, Phongluxa Khampheng, Sengchanh Kounnavong, Jun Kobayashi
{"title":"Trend of sociodemographic and economic inequalities in the use of maternal health services in Lao People's Democratic Republic from 2006 to 2017: MICS data analysis.","authors":"Noudéhouénou Credo Adelphe Ahissou, Daisuke Nonaka, Rie Takeuchi, Calvin de Los Reyes, Manami Uehara, Phongluxa Khampheng, Sengchanh Kounnavong, Jun Kobayashi","doi":"10.1186/s41182-023-00548-2","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Maternal mortalities remain high in the Lao People's Democratic Republic (Lao PDR). Since 2012, to improve access to maternal health services for all women, the country implemented several policies and strategies including user fee removal interventions for childbirth-related care. However, it remains unclear whether inequalities in access to services have reduced in the post-2012 period compared to pre-2012. Our study compared the change in sociodemographic and economic inequalities in access to maternal health services between 2006 to 2011-12 and 2011-12 to 2017.</p><p><strong>Methods: </strong>We used the three most recent Lao Social Indicator Survey datasets conducted in 2006, 2011-12, and 2017 for this analysis. We assessed wealth, area of residence, ethnicity, educational attainment, and women's age-related inequalities in the use of at least one antenatal care (ANC) visit with skilled personnel, institutional delivery, and at least one facility-based postnatal care (PNC) visit by mothers. The magnitude of inequalities was measured using concentration curves, concentration indices (CIX), and equiplots.</p><p><strong>Results: </strong>The coverage of at least one ANC with skilled personnel increased the most between 2012 and 2017, by 37.1% in Hmong minority ethnic group women, 36.1% in women living in rural areas, 31.1%, and 28.4 in the poorest and poor, respectively. In the same period, institutional deliveries increased the most among women in the middle quintiles by 32.8%, the poor by 29.3%, and Hmong women by 30.2%. The most significant reduction in inequalities was related to area of residence between 2006 and 2012 while it was based on wealth quintiles in the period 2011-12 to 2017. Finally, in 2017, wealth-related inequalities in institutional delivery remained high, with a CIX of 0.193 which was the highest of all CIX values.</p><p><strong>Conclusion: </strong>There was a significant decline in inequalities based on the area of residence in the use of maternal health services between 2006 and 2011-12 while between 2011-12 and 2017, the largest decrease was based on wealth quintiles. Policies and strategies implemented since 2011-12 might have been successful in improving access to maternal health services in Lao PDR. Meanwhile, more attention should be given to improving the uptake of facility-based PNC visits.</p>","PeriodicalId":23311,"journal":{"name":"Tropical Medicine and Health","volume":"51 1","pages":"56"},"PeriodicalIF":3.5000,"publicationDate":"2023-10-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10585846/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Tropical Medicine and Health","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s41182-023-00548-2","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"TROPICAL MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
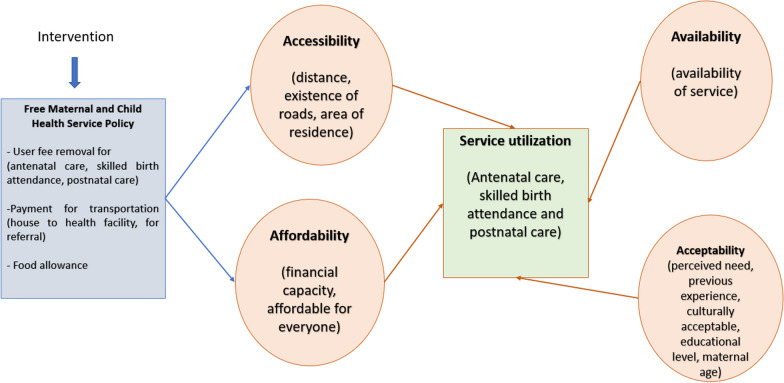
Background: Maternal mortalities remain high in the Lao People's Democratic Republic (Lao PDR). Since 2012, to improve access to maternal health services for all women, the country implemented several policies and strategies including user fee removal interventions for childbirth-related care. However, it remains unclear whether inequalities in access to services have reduced in the post-2012 period compared to pre-2012. Our study compared the change in sociodemographic and economic inequalities in access to maternal health services between 2006 to 2011-12 and 2011-12 to 2017.
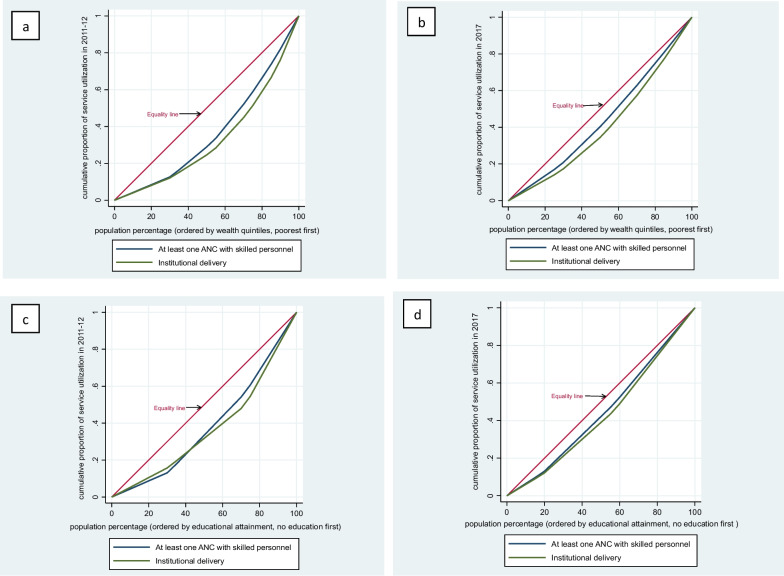
Methods: We used the three most recent Lao Social Indicator Survey datasets conducted in 2006, 2011-12, and 2017 for this analysis. We assessed wealth, area of residence, ethnicity, educational attainment, and women's age-related inequalities in the use of at least one antenatal care (ANC) visit with skilled personnel, institutional delivery, and at least one facility-based postnatal care (PNC) visit by mothers. The magnitude of inequalities was measured using concentration curves, concentration indices (CIX), and equiplots.
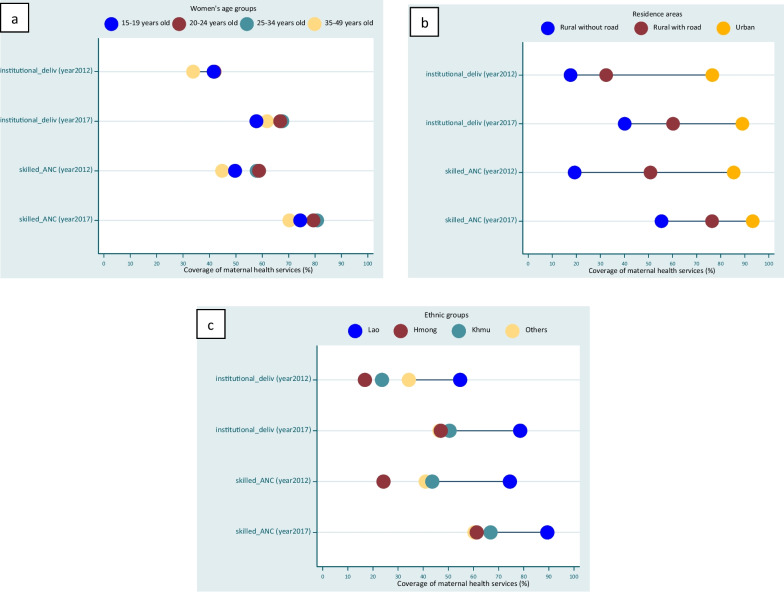
Results: The coverage of at least one ANC with skilled personnel increased the most between 2012 and 2017, by 37.1% in Hmong minority ethnic group women, 36.1% in women living in rural areas, 31.1%, and 28.4 in the poorest and poor, respectively. In the same period, institutional deliveries increased the most among women in the middle quintiles by 32.8%, the poor by 29.3%, and Hmong women by 30.2%. The most significant reduction in inequalities was related to area of residence between 2006 and 2012 while it was based on wealth quintiles in the period 2011-12 to 2017. Finally, in 2017, wealth-related inequalities in institutional delivery remained high, with a CIX of 0.193 which was the highest of all CIX values.
Conclusion: There was a significant decline in inequalities based on the area of residence in the use of maternal health services between 2006 and 2011-12 while between 2011-12 and 2017, the largest decrease was based on wealth quintiles. Policies and strategies implemented since 2011-12 might have been successful in improving access to maternal health services in Lao PDR. Meanwhile, more attention should be given to improving the uptake of facility-based PNC visits.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
