{"title":"Predicting acute kidney injury with an artificial intelligence-driven model in a pediatric cardiac intensive care unit.","authors":"Tiziana Fragasso, Valeria Raggi, Davide Passaro, Luca Tardella, Giovanna Jona Lasinio, Zaccaria Ricci","doi":"10.1186/s44158-023-00125-3","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Acute kidney injury (AKI) is among the most common complications following cardiac surgery in adult and pediatric patients, significantly affecting morbidity and mortality. Artificial Intelligence (AI) with Machine Learning (ML) can be used to predict outcomes. AKI diagnosis anticipation may be an ideal target of these methods. The scope of the study is building a Machine Learning (ML) train model with Random Forest (RF) algorithm, based on electronic health record (EHR) data, able to forecast AKI continuously after 48 h in post-cardiac surgery children, and to test its performance. Four hundred nineteen consecutive patients out of 1115 hospital admissions were enrolled in a single-center retrospective study. Patients were younger than 18 years and admitted from August 2018 to February 2020 in a pediatric cardiac intensive care unit (PCICU) undergoing cardiac surgery, invasive procedure (hemodynamic studies), and medical conditions with complete EHR records and discharged after 48 h or more.</p><p><strong>Results: </strong>Thirty-six variables were selected to build the algorithm according to commonly described cardiac surgery-associated AKI clinical predictors. We evaluated different models for different outcomes: binary AKI (no AKI vs. AKI), severe AKI (no-mild vs severe AKI), and multiclass classification (maximum AKI and the most frequent level of AKI, mode AKI). The algorithm performance was assessed with the area under the curve receiver operating characteristics (AUC ROC) for binary classification, with accuracy and K for multiclass classification. AUC ROC for binary AKI was 0.93 (95% CI 0.92-0.94), and for severe AKI was 0.99 (95% CI 0.98-1). Mode AKI accuracy was 0.95, and K was 0.80 (95% CI 0.94-0.96); maximum AKI accuracy was 0.92, and K was 0.71 (95% CI 0.91-0.93). The importance matrix plot demonstrated creatinine, basal creatinine, platelets count, adrenaline support, and lactate dehydrogenase for binary AKI with the addition of cardiopulmonary bypass duration for severe AKI as the most relevant variables of the model.</p><p><strong>Conclusions: </strong>We validated a ML model to detect AKI occurring after 48 h in a retrospective observational study that could help clinicians in individuating patients at risk of AKI, in which a preventive strategy can be determinant to improve the occurrence of renal dysfunction.</p>","PeriodicalId":73597,"journal":{"name":"Journal of Anesthesia, Analgesia and Critical Care (Online)","volume":"3 1","pages":"37"},"PeriodicalIF":3.1000,"publicationDate":"2023-10-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10583404/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Anesthesia, Analgesia and Critical Care (Online)","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s44158-023-00125-3","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
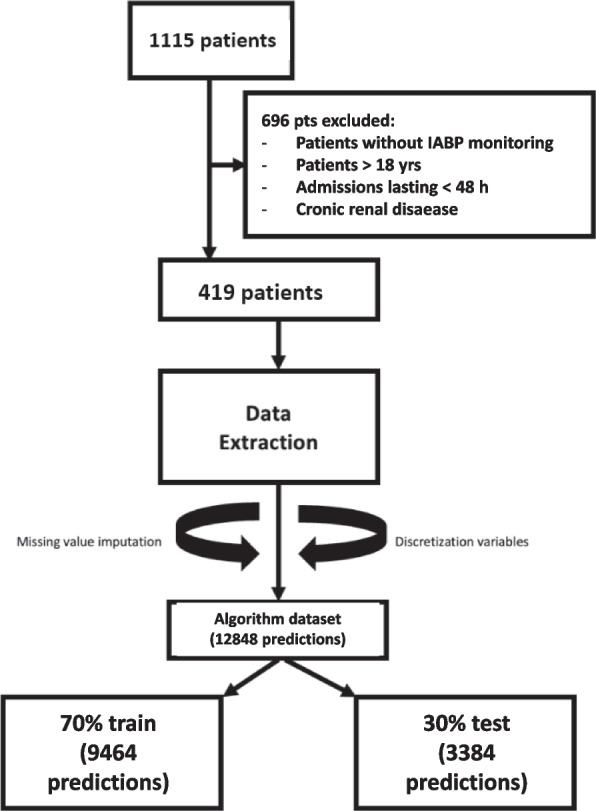
Background: Acute kidney injury (AKI) is among the most common complications following cardiac surgery in adult and pediatric patients, significantly affecting morbidity and mortality. Artificial Intelligence (AI) with Machine Learning (ML) can be used to predict outcomes. AKI diagnosis anticipation may be an ideal target of these methods. The scope of the study is building a Machine Learning (ML) train model with Random Forest (RF) algorithm, based on electronic health record (EHR) data, able to forecast AKI continuously after 48 h in post-cardiac surgery children, and to test its performance. Four hundred nineteen consecutive patients out of 1115 hospital admissions were enrolled in a single-center retrospective study. Patients were younger than 18 years and admitted from August 2018 to February 2020 in a pediatric cardiac intensive care unit (PCICU) undergoing cardiac surgery, invasive procedure (hemodynamic studies), and medical conditions with complete EHR records and discharged after 48 h or more.
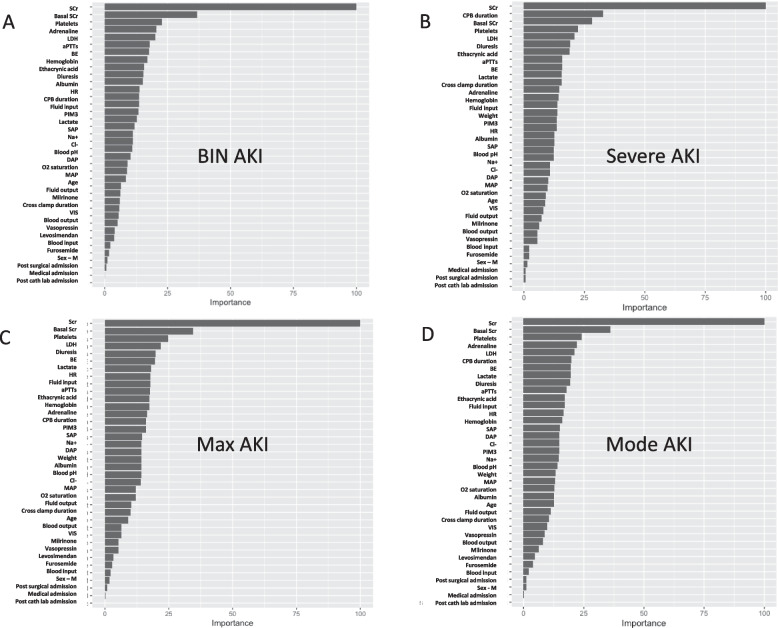
Results: Thirty-six variables were selected to build the algorithm according to commonly described cardiac surgery-associated AKI clinical predictors. We evaluated different models for different outcomes: binary AKI (no AKI vs. AKI), severe AKI (no-mild vs severe AKI), and multiclass classification (maximum AKI and the most frequent level of AKI, mode AKI). The algorithm performance was assessed with the area under the curve receiver operating characteristics (AUC ROC) for binary classification, with accuracy and K for multiclass classification. AUC ROC for binary AKI was 0.93 (95% CI 0.92-0.94), and for severe AKI was 0.99 (95% CI 0.98-1). Mode AKI accuracy was 0.95, and K was 0.80 (95% CI 0.94-0.96); maximum AKI accuracy was 0.92, and K was 0.71 (95% CI 0.91-0.93). The importance matrix plot demonstrated creatinine, basal creatinine, platelets count, adrenaline support, and lactate dehydrogenase for binary AKI with the addition of cardiopulmonary bypass duration for severe AKI as the most relevant variables of the model.
Conclusions: We validated a ML model to detect AKI occurring after 48 h in a retrospective observational study that could help clinicians in individuating patients at risk of AKI, in which a preventive strategy can be determinant to improve the occurrence of renal dysfunction.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
