Jesse Fishman, Seri Anderson, Sandra E Talbird, David Dingli
{"title":"Analysis of Costs per Responder in US Adults with Paroxysmal Nocturnal Hemoglobinuria with a Suboptimal Response to Prior Eculizumab Treatment.","authors":"Jesse Fishman, Seri Anderson, Sandra E Talbird, David Dingli","doi":"10.3390/hematolrep15040060","DOIUrl":null,"url":null,"abstract":"<p><p>European Society for Blood and Marrow Transplantation (EBMT) hematologic response categories comprehensively assess complement inhibitor responses in patients with paroxysmal nocturnal hemoglobinuria (PNH). Using data from the 16-week randomized controlled period of the phase 3 PEGASUS trial (N = 80), we estimated the treatment cost per responder by the EBMT response category for pegcetacoplan and eculizumab in adults with PNH and a suboptimal response to eculizumab. Average drug costs per responder, number needed to treat, and incremental drug costs per responder were estimated using dosages administered during the trial (base case). A US payer perspective (2020 US dollars) was used. Scenario analyses were conducted for various costs, dosages, treatment durations, patient populations, and settings. In total, 30 of 41 (73%) who switched to pegcetacoplan and 2 of 39 (5%) patients who continued eculizumab had a good, major, or complete response (good-to-complete responders) at Week 16. Average weekly drug costs per good-to-complete responder were USD 15,923 with pegcetacoplan and USD 216,100 with eculizumab; average weekly drug costs per patient were USD 11,651 and USD 11,082, respectively. Average drug costs per good-to-complete responder with pegcetacoplan were similar across complement inhibitor-naïve populations and were consistently lower than with eculizumab. Switching from eculizumab to pegcetacoplan allowed more patients with a suboptimal response to attain a good-to-complete response at lower costs. These results apply to patients with a suboptimal response to prior eculizumab treatment only.</p>","PeriodicalId":12829,"journal":{"name":"Hematology Reports","volume":"15 4","pages":"578-591"},"PeriodicalIF":1.2000,"publicationDate":"2023-10-13","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10594490/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Hematology Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3390/hematolrep15040060","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"HEMATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
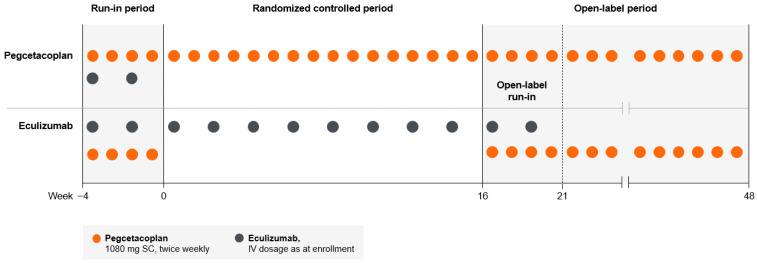
European Society for Blood and Marrow Transplantation (EBMT) hematologic response categories comprehensively assess complement inhibitor responses in patients with paroxysmal nocturnal hemoglobinuria (PNH). Using data from the 16-week randomized controlled period of the phase 3 PEGASUS trial (N = 80), we estimated the treatment cost per responder by the EBMT response category for pegcetacoplan and eculizumab in adults with PNH and a suboptimal response to eculizumab. Average drug costs per responder, number needed to treat, and incremental drug costs per responder were estimated using dosages administered during the trial (base case). A US payer perspective (2020 US dollars) was used. Scenario analyses were conducted for various costs, dosages, treatment durations, patient populations, and settings. In total, 30 of 41 (73%) who switched to pegcetacoplan and 2 of 39 (5%) patients who continued eculizumab had a good, major, or complete response (good-to-complete responders) at Week 16. Average weekly drug costs per good-to-complete responder were USD 15,923 with pegcetacoplan and USD 216,100 with eculizumab; average weekly drug costs per patient were USD 11,651 and USD 11,082, respectively. Average drug costs per good-to-complete responder with pegcetacoplan were similar across complement inhibitor-naïve populations and were consistently lower than with eculizumab. Switching from eculizumab to pegcetacoplan allowed more patients with a suboptimal response to attain a good-to-complete response at lower costs. These results apply to patients with a suboptimal response to prior eculizumab treatment only.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
