Celeste A Green, Jasmine D Johnson, Christine McKenzie, Alison M Stuebe
{"title":"Standardized Order Sets Do Not Eliminate Racial or Ethnic Inequities in Postpartum Pain Management.","authors":"Celeste A Green, Jasmine D Johnson, Christine McKenzie, Alison M Stuebe","doi":"10.1089/heq.2022.0180","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>To quantify the extent to which a standardized pain management order set reduced racial and ethnic inequities in post-cesarean pain evaluation and management.</p><p><strong>Methods: </strong>We conducted a retrospective cohort study to quantify racial and ethnic differences in pain evaluation and management before (July 2014-June 2016) and after implementation of a standardized post-cesarean order set (March 2017-February 2018). Electronic medical records were queried for pain scores >7/10, number of pain assessments, and opioid, nonsteroidal anti-inflammatory drug (NSAID), and acetaminophen doses. Outcomes were grouped into 0 to <24 and 24-48 h postpartum, and stratified by race/ethnicity (Hispanic, non-Hispanic Black [NHB], non-Hispanic White [NHW], Asian, and other), as documented in the electronic health record. Analyses included logistic regression for the categorical outcome of pain score >7 (severe pain), and linear regression, with propensity score adjustment. Main effect and interaction terms were used to calculate the difference-in-difference in pain process and outcome measures between the baseline and follow-up periods.</p><p><strong>Results: </strong>After order set implementation (<i>N</i>=888), severe pain remained more common among NHB patients (% pain scores >7 NHW vs. NHB 0 to <24 h: 22% vs. 33%, <i>p</i>=0.003; 24-48 h: 26% vs. 40%, <i>p</i><0.001). Among all patients, pain management processes changed after implementation of the order set, with overall fewer assessments, less Opioids, and more nonopioid analgesics. However, racial and ethnic inequities in a number of assessments and in treatment were unchanged (all <i>p</i> for interaction >0.05), with the exception of a modest increase in NSAID doses 24-48 h postpartum for Hispanic patients.</p><p><strong>Conclusion: </strong>A standardized pain management order set reduced overall postpartum opioid use, but did not reduce racial and ethnic disparities in pain evaluation and management. Future work should investigate racial equity-focused education and interventions designed to eliminate disparities in pain management.</p>","PeriodicalId":36602,"journal":{"name":"Health Equity","volume":"7 1","pages":"685-691"},"PeriodicalIF":2.5000,"publicationDate":"2023-10-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10615045/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Health Equity","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1089/heq.2022.0180","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"PUBLIC, ENVIRONMENTAL & OCCUPATIONAL HEALTH","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: To quantify the extent to which a standardized pain management order set reduced racial and ethnic inequities in post-cesarean pain evaluation and management.
Methods: We conducted a retrospective cohort study to quantify racial and ethnic differences in pain evaluation and management before (July 2014-June 2016) and after implementation of a standardized post-cesarean order set (March 2017-February 2018). Electronic medical records were queried for pain scores >7/10, number of pain assessments, and opioid, nonsteroidal anti-inflammatory drug (NSAID), and acetaminophen doses. Outcomes were grouped into 0 to <24 and 24-48 h postpartum, and stratified by race/ethnicity (Hispanic, non-Hispanic Black [NHB], non-Hispanic White [NHW], Asian, and other), as documented in the electronic health record. Analyses included logistic regression for the categorical outcome of pain score >7 (severe pain), and linear regression, with propensity score adjustment. Main effect and interaction terms were used to calculate the difference-in-difference in pain process and outcome measures between the baseline and follow-up periods.
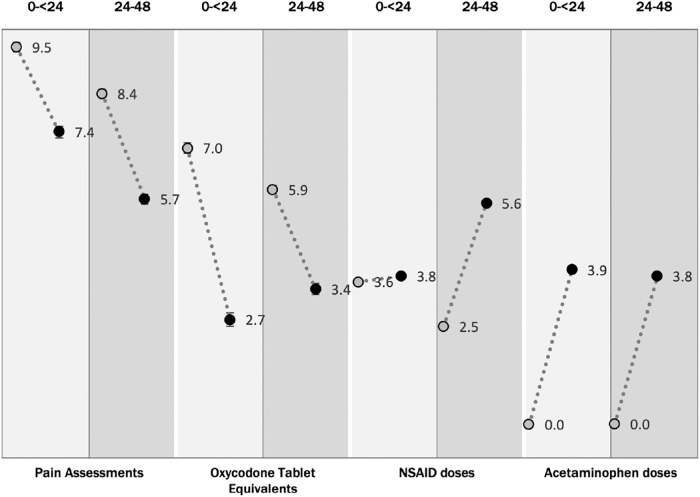
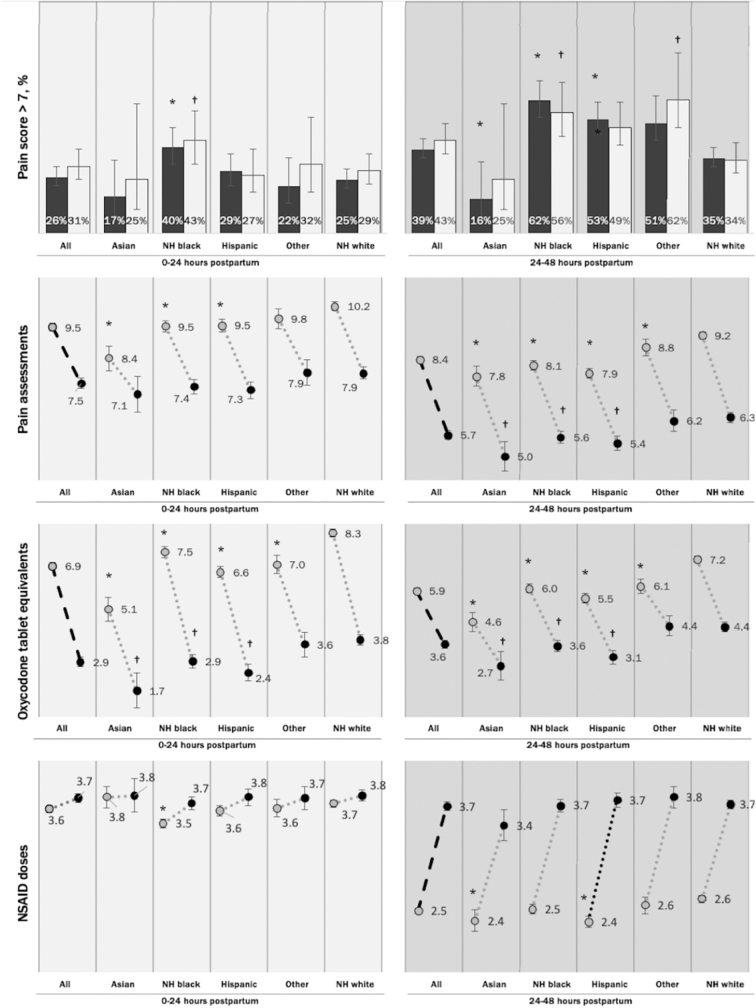
Results: After order set implementation (N=888), severe pain remained more common among NHB patients (% pain scores >7 NHW vs. NHB 0 to <24 h: 22% vs. 33%, p=0.003; 24-48 h: 26% vs. 40%, p<0.001). Among all patients, pain management processes changed after implementation of the order set, with overall fewer assessments, less Opioids, and more nonopioid analgesics. However, racial and ethnic inequities in a number of assessments and in treatment were unchanged (all p for interaction >0.05), with the exception of a modest increase in NSAID doses 24-48 h postpartum for Hispanic patients.
Conclusion: A standardized pain management order set reduced overall postpartum opioid use, but did not reduce racial and ethnic disparities in pain evaluation and management. Future work should investigate racial equity-focused education and interventions designed to eliminate disparities in pain management.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
