Michael Bogart, Carl B Abbott, Mohan Bangalore, Donna McMorrow, Elizabeth R Packnett, Kristi DiRocco
{"title":"Changes in Oral Corticosteroid Utilization in Patients with COPD Following Initiation of FF/UMEC/VI.","authors":"Michael Bogart, Carl B Abbott, Mohan Bangalore, Donna McMorrow, Elizabeth R Packnett, Kristi DiRocco","doi":"10.2147/COPD.S419272","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>Oral corticosteroids (OCS) play a role in the treatment of acute chronic obstructive pulmonary disease (COPD) exacerbations; however, chronic use is not recommended due to the high rate of systemic complications, development of comorbidities, and increased mortality. Data assessing the real-world impact of fluticasone furoate/umeclidinium/vilanterol (FF/UMEC/VI) on OCS utilization rates are limited. This study assessed the impact of FF/UMEC/VI on OCS use among patients with COPD previously treated with OCS.</p><p><strong>Patients and methods: </strong>A retrospective database study of patients with COPD aged ≥40 years who initiated FF/UMEC/VI from 1 November 2017 to 31 December 2018, identified through the MarketScan<sup>®</sup> Commercial and Medicare Supplemental databases. Patients were required to have ≥1 dispensing of an OCS prior to initiation of FF/UMEC/VI (index) and were followed up for 12 months post-index. OCS utilization patterns, potential OCS-related adverse events, healthcare resource utilization (HCRU), and costs were compared between the 12-month pre- and post-index periods.</p><p><strong>Results: </strong>A total of 2013 patients were identified (mean age 63.5 years, 55.7% female). The proportion of patients with ≥1 OCS claim decreased by 32.2% between the pre- and post-index period (67.8% vs 100%; p < 0.001). Comparing the post-index period to the pre-index period, mean number of OCS pharmacy claims per patient decreased from 3.3 to 2.5 (p < 0.001) and mean daily dose was reduced from 3.1 to 2.6 mg/day (p = 0.004); 30.0% of patients reduced their daily dose by 90-100%. Reductions were also seen in COPD-related HCRU. The proportion of patients with an inpatient admission for COPD decreased from 11.4% to 7.1% (p < 0.001), emergency room visits decreased from 23.1% to 17.4% (p < 0.001), and office visits from 97.5% to 90.1% (p < 0.001). Similar results were seen for all-cause HCRU.</p><p><strong>Conclusion: </strong>Among patients with COPD with prior OCS use, FF/UMEC/VI initiation resulted in significant reductions in OCS utilization, COPD-related HCRU (including hospitalization), and all-cause HCRU.</p>","PeriodicalId":48818,"journal":{"name":"International Journal of Chronic Obstructive Pulmonary Disease","volume":"18 ","pages":"2367-2379"},"PeriodicalIF":3.1000,"publicationDate":"2023-11-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10625739/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Journal of Chronic Obstructive Pulmonary Disease","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.2147/COPD.S419272","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"RESPIRATORY SYSTEM","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose: Oral corticosteroids (OCS) play a role in the treatment of acute chronic obstructive pulmonary disease (COPD) exacerbations; however, chronic use is not recommended due to the high rate of systemic complications, development of comorbidities, and increased mortality. Data assessing the real-world impact of fluticasone furoate/umeclidinium/vilanterol (FF/UMEC/VI) on OCS utilization rates are limited. This study assessed the impact of FF/UMEC/VI on OCS use among patients with COPD previously treated with OCS.
Patients and methods: A retrospective database study of patients with COPD aged ≥40 years who initiated FF/UMEC/VI from 1 November 2017 to 31 December 2018, identified through the MarketScan® Commercial and Medicare Supplemental databases. Patients were required to have ≥1 dispensing of an OCS prior to initiation of FF/UMEC/VI (index) and were followed up for 12 months post-index. OCS utilization patterns, potential OCS-related adverse events, healthcare resource utilization (HCRU), and costs were compared between the 12-month pre- and post-index periods.
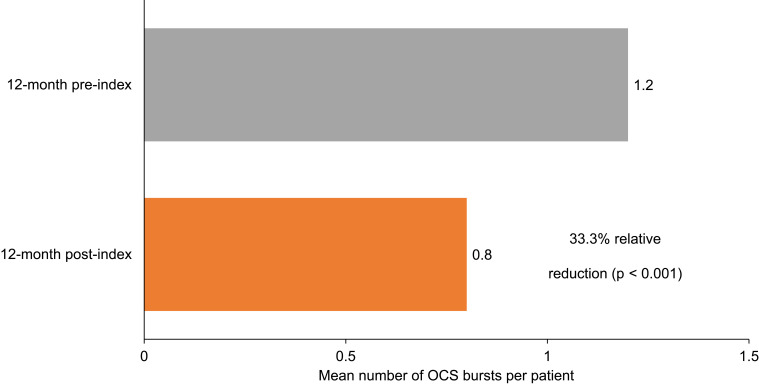
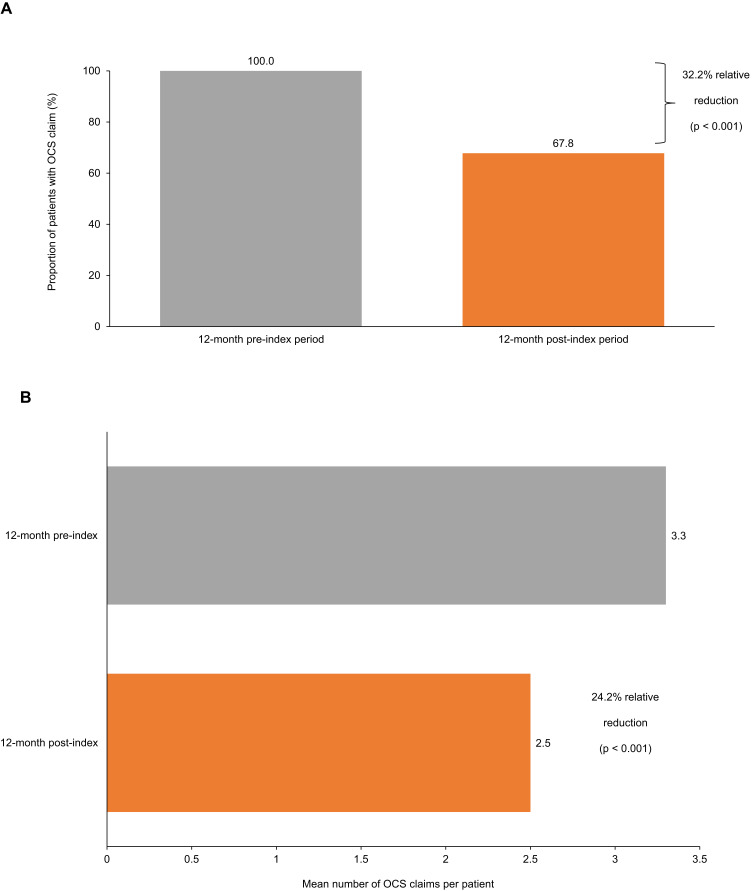
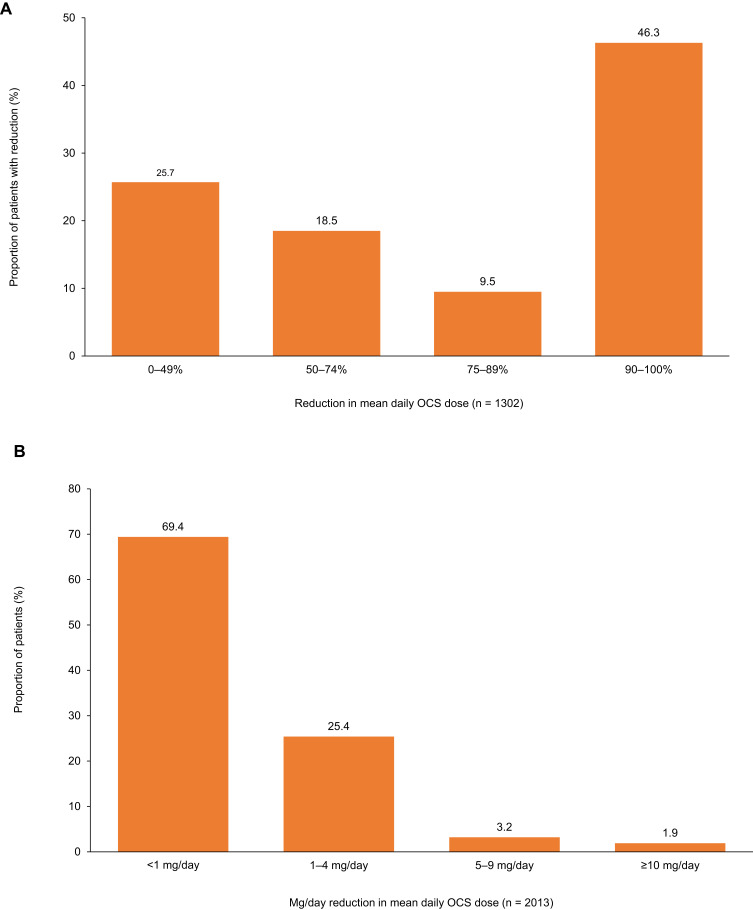
Results: A total of 2013 patients were identified (mean age 63.5 years, 55.7% female). The proportion of patients with ≥1 OCS claim decreased by 32.2% between the pre- and post-index period (67.8% vs 100%; p < 0.001). Comparing the post-index period to the pre-index period, mean number of OCS pharmacy claims per patient decreased from 3.3 to 2.5 (p < 0.001) and mean daily dose was reduced from 3.1 to 2.6 mg/day (p = 0.004); 30.0% of patients reduced their daily dose by 90-100%. Reductions were also seen in COPD-related HCRU. The proportion of patients with an inpatient admission for COPD decreased from 11.4% to 7.1% (p < 0.001), emergency room visits decreased from 23.1% to 17.4% (p < 0.001), and office visits from 97.5% to 90.1% (p < 0.001). Similar results were seen for all-cause HCRU.
Conclusion: Among patients with COPD with prior OCS use, FF/UMEC/VI initiation resulted in significant reductions in OCS utilization, COPD-related HCRU (including hospitalization), and all-cause HCRU.
期刊介绍:
An international, peer-reviewed journal of therapeutics and pharmacology focusing on concise rapid reporting of clinical studies and reviews in COPD. Special focus will be given to the pathophysiological processes underlying the disease, intervention programs, patient focused education, and self management protocols. This journal is directed at specialists and healthcare professionals



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
