Jonathan P Wong, Kyle Runeckles, Cedric Manlhiot, Sunita O'Shea, Tanveer Collins, Bailey Bernknopf, Pedrom Farid, Nita Chahal, Brian W McCrindle
{"title":"Socioeconomic Status and Kawasaki Disease Outcomes in a Single-Payer Health Care System.","authors":"Jonathan P Wong, Kyle Runeckles, Cedric Manlhiot, Sunita O'Shea, Tanveer Collins, Bailey Bernknopf, Pedrom Farid, Nita Chahal, Brian W McCrindle","doi":"10.1016/j.cjcpc.2022.10.007","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>For patients with Kawasaki disease (KD), lower socioeconomic status (SES) may adversely affect the timeliness of presentation and initiation of intravenous immune globulin, and coronary artery outcomes. Multipayer systems have been shown to affect health care equity and access to health care negatively. We sought to determine the association of SES with KD outcomes in a single-payer health care system.</p><p><strong>Methods: </strong>Patients with KD presenting from 2007 to 2017 at a single institution were included. SES data were obtained by matching patient postal code district with data from the 2016 Census Canada.</p><p><strong>Results: </strong>SES data were linked for 1018 patients. The proportion of households living below the after-tax low-income cutoff in the patient's postal code district was 13% for not treated, 13% for delayed intravenous immune globulin treatment, and 12% for prompt treatment (<i>P</i> = 0.58). Likewise, the average median annual household income was unrelated to delayed or no treatment. The percentage >15 years of age with advanced education differed between groups at 33%, 29%, and 31% for delayed treatment, prompt treatment, and missed groups, respectively (<i>P</i> = 0.004). SES variables were not significantly different for those with vs without coronary artery aneurysms (max Z-score: >2.5), including the proportion of households living below low-income cutoff (12% vs 13%; <i>P</i> = 0.37), average median annual household income (CAD$81,220 vs $82,055; <i>P</i> = 0.78), and proportion with a university degree (33% vs 31%; <i>P</i> = 0.49), even after adjusting for sex, age, year, and KD type.</p><p><strong>Conclusions: </strong>Timeliness of treatment for KD and coronary artery outcomes were not associated with SES variables within a single-payer health care system.</p>","PeriodicalId":11447,"journal":{"name":"Duke Mathematical Journal","volume":"61 1","pages":"248-252"},"PeriodicalIF":3.0000,"publicationDate":"2022-11-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10642103/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Duke Mathematical Journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1016/j.cjcpc.2022.10.007","RegionNum":1,"RegionCategory":"数学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/12/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"MATHEMATICS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: For patients with Kawasaki disease (KD), lower socioeconomic status (SES) may adversely affect the timeliness of presentation and initiation of intravenous immune globulin, and coronary artery outcomes. Multipayer systems have been shown to affect health care equity and access to health care negatively. We sought to determine the association of SES with KD outcomes in a single-payer health care system.
Methods: Patients with KD presenting from 2007 to 2017 at a single institution were included. SES data were obtained by matching patient postal code district with data from the 2016 Census Canada.
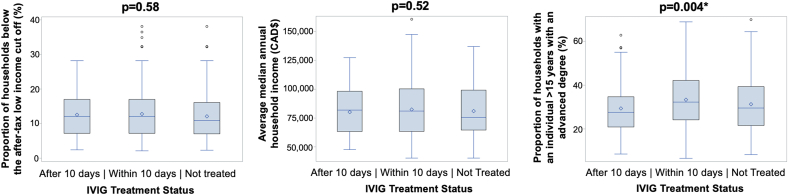
Results: SES data were linked for 1018 patients. The proportion of households living below the after-tax low-income cutoff in the patient's postal code district was 13% for not treated, 13% for delayed intravenous immune globulin treatment, and 12% for prompt treatment (P = 0.58). Likewise, the average median annual household income was unrelated to delayed or no treatment. The percentage >15 years of age with advanced education differed between groups at 33%, 29%, and 31% for delayed treatment, prompt treatment, and missed groups, respectively (P = 0.004). SES variables were not significantly different for those with vs without coronary artery aneurysms (max Z-score: >2.5), including the proportion of households living below low-income cutoff (12% vs 13%; P = 0.37), average median annual household income (CAD$81,220 vs $82,055; P = 0.78), and proportion with a university degree (33% vs 31%; P = 0.49), even after adjusting for sex, age, year, and KD type.
Conclusions: Timeliness of treatment for KD and coronary artery outcomes were not associated with SES variables within a single-payer health care system.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
