Amanda P C S Boteon, Marisa R D Lima, Bianca Della Guardia, Mauricio F Carvalho, Andrea Schlegel, Yuri L Boteon
{"title":"Establishing a HOPE Program in a Real-life Setting: A Brazilian Case Series.","authors":"Amanda P C S Boteon, Marisa R D Lima, Bianca Della Guardia, Mauricio F Carvalho, Andrea Schlegel, Yuri L Boteon","doi":"10.1097/TXD.0000000000001555","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Although hypothermic oxygenated perfusion (HOPE) improves posttransplant outcomes, setting up machine perfusion programs may be subjected to specific obstacles under different conditions. This study aims to describe the establishment of HOPE in a real-life setting in Brazil.</p><p><strong>Methods: </strong>Extended criteria donors in donation after brain death organs preserved by HOPE were accepted for higher-risk candidates needing expedited transplantation, perceived as those who would benefit most from the technique because of its limited availability. Extended criteria donors was defined by the Eurotransplant criteria. High-risk transplant candidates were characterized by suboptimal surgical conditions related to the recipient or the procedure.</p><p><strong>Results: </strong>Six HOPE-preserved grafts were transplanted from February 2022 to August 2022. The mean donor risk index was 1.7 (SD 0.5). One organ was severely steatotic, and 3 had an anticipated cold ischemia time above 12 h. Recipients' mean model for end-stage liver disease was 28.67 (SD 6.79), with 1 case of retransplant, 1 of refractory ascites, and 1 of acute-on-chronic liver failure. The mean cold ischemia time was 5 h 42 min (SD 82 min), HOPE 6 h 3 min (SD 150 min), and total preservation time 11 h 46 min (SD 184 min). No case had early allograft dysfunction. The mean length of hospital stay was 10 d with 100% graft and patient survival and no ischemic cholangiopathies at a median follow-up of 15 mo (min 12, max 18). Costs and country-specific legal regulations for device utilization were the major hurdles to implementing the program.</p><p><strong>Conclusion: </strong>We presented a pathway to introduce and rationalize the use of HOPE in a scenario of challenging donor-recipient matching with good results. These findings may aid in implementing machine perfusion programs, especially in settings with limited resources or complex transplant logistics.</p>","PeriodicalId":23225,"journal":{"name":"Transplantation Direct","volume":"9 12","pages":"e1555"},"PeriodicalIF":1.9000,"publicationDate":"2023-11-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10635603/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Transplantation Direct","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/TXD.0000000000001555","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/12/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"TRANSPLANTATION","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Although hypothermic oxygenated perfusion (HOPE) improves posttransplant outcomes, setting up machine perfusion programs may be subjected to specific obstacles under different conditions. This study aims to describe the establishment of HOPE in a real-life setting in Brazil.
Methods: Extended criteria donors in donation after brain death organs preserved by HOPE were accepted for higher-risk candidates needing expedited transplantation, perceived as those who would benefit most from the technique because of its limited availability. Extended criteria donors was defined by the Eurotransplant criteria. High-risk transplant candidates were characterized by suboptimal surgical conditions related to the recipient or the procedure.
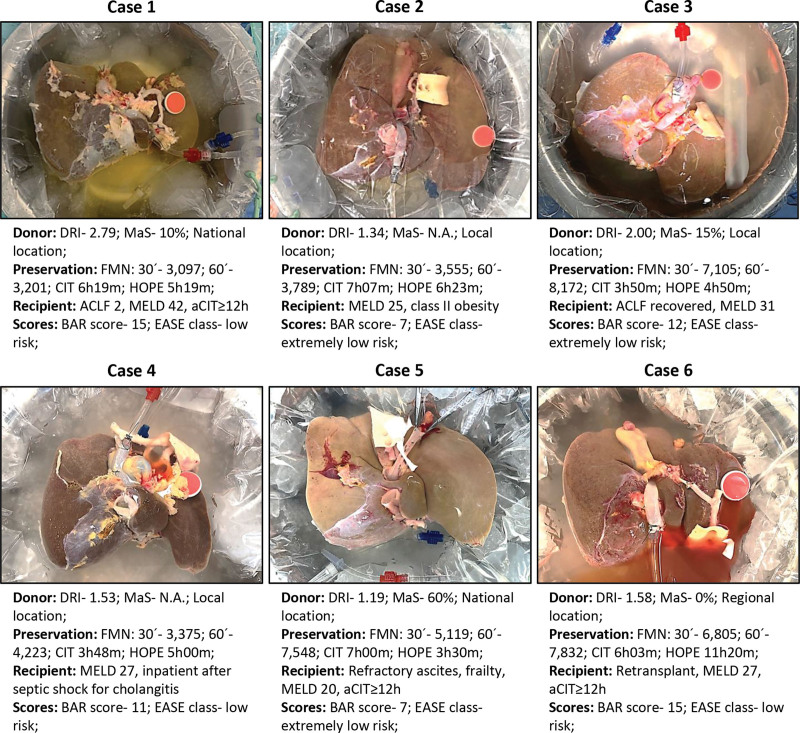
Results: Six HOPE-preserved grafts were transplanted from February 2022 to August 2022. The mean donor risk index was 1.7 (SD 0.5). One organ was severely steatotic, and 3 had an anticipated cold ischemia time above 12 h. Recipients' mean model for end-stage liver disease was 28.67 (SD 6.79), with 1 case of retransplant, 1 of refractory ascites, and 1 of acute-on-chronic liver failure. The mean cold ischemia time was 5 h 42 min (SD 82 min), HOPE 6 h 3 min (SD 150 min), and total preservation time 11 h 46 min (SD 184 min). No case had early allograft dysfunction. The mean length of hospital stay was 10 d with 100% graft and patient survival and no ischemic cholangiopathies at a median follow-up of 15 mo (min 12, max 18). Costs and country-specific legal regulations for device utilization were the major hurdles to implementing the program.
Conclusion: We presented a pathway to introduce and rationalize the use of HOPE in a scenario of challenging donor-recipient matching with good results. These findings may aid in implementing machine perfusion programs, especially in settings with limited resources or complex transplant logistics.
背景:虽然低温氧灌注(hypothermic oxygenated perfusion, HOPE)可以改善移植后的预后,但在不同情况下,设置机器灌注程序可能会遇到特定的障碍。本研究旨在描述希望在巴西现实生活中的建立。方法:对于需要加速移植的高风险候选人,接受由HOPE保存的脑死亡后器官捐赠的扩展标准供者,因为其有限的可用性,被认为是那些将从该技术中获益最多的人。扩展标准供体由欧洲移植标准定义。高危移植候选者的特点是与受体或手术相关的次优手术条件。结果:2022年2月至2022年8月,6例保存希望的移植物移植。平均供者风险指数为1.7 (SD 0.5)。1个器官严重脂肪变性,3个预计冷缺血时间超过12小时。受者终末期肝病的平均模型为28.67例(SD 6.79),再移植1例,难治性腹水1例,急性慢性肝衰竭1例。平均冷缺血时间为5 h 42 min (SD 82 min), HOPE为6 h 3 min (SD 150 min),总保存时间为11 h 46 min (SD 184 min)。无一例出现早期同种异体移植物功能障碍。平均住院时间为10天,移植100%,患者存活率为100%,中位随访15个月(最短12个月,最长18个月)无缺血性胆管病变。成本和国家特定的设备使用法律法规是实施该计划的主要障碍。结论:我们提出了在具有挑战性的供体-受体匹配场景中引入和合理化HOPE使用的途径,并取得了良好的效果。这些发现可能有助于实施机器灌注方案,特别是在资源有限或移植后勤复杂的情况下。



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
