Primary radiotherapy and deep inferior epigastric perforator flap reconstruction for patients with breast cancer (PRADA): a multicentre, prospective, non-randomised, feasibility study.
Paul T R Thiruchelvam, Daniel R Leff, Amy R Godden, Susan Cleator, Simon H Wood, Anna M Kirby, Navid Jallali, Navita Somaiah, Judith E Hunter, Francis P Henry, Aikaterini Micha, Rachel L O'Connell, Kabir Mohammed, Neill Patani, Melissa L H Tan, Dorothy Gujral, Gillian Ross, Stuart E James, Aadil A Khan, Jennifer E Rusby, Dimitri J Hadjiminas, Fiona A MacNeill
{"title":"Primary radiotherapy and deep inferior epigastric perforator flap reconstruction for patients with breast cancer (PRADA): a multicentre, prospective, non-randomised, feasibility study.","authors":"Paul T R Thiruchelvam, Daniel R Leff, Amy R Godden, Susan Cleator, Simon H Wood, Anna M Kirby, Navid Jallali, Navita Somaiah, Judith E Hunter, Francis P Henry, Aikaterini Micha, Rachel L O'Connell, Kabir Mohammed, Neill Patani, Melissa L H Tan, Dorothy Gujral, Gillian Ross, Stuart E James, Aadil A Khan, Jennifer E Rusby, Dimitri J Hadjiminas, Fiona A MacNeill","doi":"10.1016/S1470-2045(22)00145-0","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Radiotherapy before mastectomy and autologous free-flap breast reconstruction can avoid adverse radiation effects on healthy donor tissues and delays to adjuvant radiotherapy. However, evidence for this treatment sequence is sparse. We aimed to explore the feasibility of preoperative radiotherapy followed by skin-sparing mastectomy and deep inferior epigastric perforator (DIEP) flap reconstruction in patients with breast cancer requiring mastectomy.</p><p><strong>Methods: </strong>We conducted a prospective, non-randomised, feasibility study at two National Health Service trusts in the UK. Eligible patients were women aged older than 18 years with a laboratory diagnosis of primary breast cancer requiring mastectomy and post-mastectomy radiotherapy, who were suitable for DIEP flap reconstruction. Preoperative radiotherapy started 3-4 weeks after neoadjuvant chemotherapy and was delivered to the breast, plus regional nodes as required, at 40 Gy in 15 fractions (over 3 weeks) or 42·72 Gy in 16 fractions (over 3·2 weeks). Adverse skin radiation toxicity was assessed preoperatively using the Radiation Therapy Oncology Group toxicity grading system. Skin-sparing mastectomy and DIEP flap reconstruction were planned for 2-6 weeks after completion of preoperative radiotherapy. The primary endpoint was the proportion of open breast wounds greater than 1 cm width requiring a dressing at 4 weeks after surgery, assessed in all participants. This study is registered with ClinicalTrials.gov, NCT02771938, and is closed to recruitment.</p><p><strong>Findings: </strong>Between Jan 25, 2016, and Dec 11, 2017, 33 patients were enrolled. At 4 weeks after surgery, four (12·1%, 95% CI 3·4-28·2) of 33 patients had an open breast wound greater than 1 cm. One (3%) patient had confluent moist desquamation (grade 3). There were no serious treatment-related adverse events and no treatment-related deaths.</p><p><strong>Interpretation: </strong>Preoperative radiotherapy followed by skin-sparing mastectomy and immediate DIEP flap reconstruction is feasible and technically safe, with rates of breast open wounds similar to those reported with post-mastectomy radiotherapy. A randomised trial comparing preoperative radiotherapy with post-mastectomy radiotherapy is required to precisely determine and compare surgical, oncological, and breast reconstruction outcomes, including quality of life.</p><p><strong>Funding: </strong>Cancer Research UK, National Institute for Health Research.</p>","PeriodicalId":73510,"journal":{"name":"Iranian journal of cancer prevention","volume":"9 1","pages":"682-690"},"PeriodicalIF":0.0000,"publicationDate":"2022-05-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9630150/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Iranian journal of cancer prevention","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1016/S1470-2045(22)00145-0","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/4/7 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Radiotherapy before mastectomy and autologous free-flap breast reconstruction can avoid adverse radiation effects on healthy donor tissues and delays to adjuvant radiotherapy. However, evidence for this treatment sequence is sparse. We aimed to explore the feasibility of preoperative radiotherapy followed by skin-sparing mastectomy and deep inferior epigastric perforator (DIEP) flap reconstruction in patients with breast cancer requiring mastectomy.
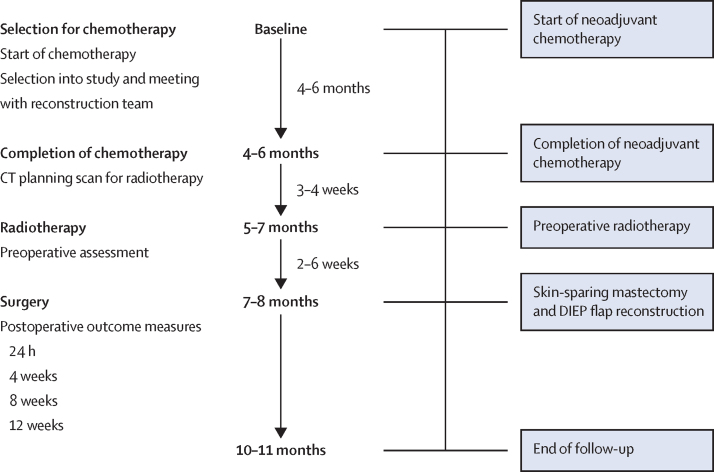
Methods: We conducted a prospective, non-randomised, feasibility study at two National Health Service trusts in the UK. Eligible patients were women aged older than 18 years with a laboratory diagnosis of primary breast cancer requiring mastectomy and post-mastectomy radiotherapy, who were suitable for DIEP flap reconstruction. Preoperative radiotherapy started 3-4 weeks after neoadjuvant chemotherapy and was delivered to the breast, plus regional nodes as required, at 40 Gy in 15 fractions (over 3 weeks) or 42·72 Gy in 16 fractions (over 3·2 weeks). Adverse skin radiation toxicity was assessed preoperatively using the Radiation Therapy Oncology Group toxicity grading system. Skin-sparing mastectomy and DIEP flap reconstruction were planned for 2-6 weeks after completion of preoperative radiotherapy. The primary endpoint was the proportion of open breast wounds greater than 1 cm width requiring a dressing at 4 weeks after surgery, assessed in all participants. This study is registered with ClinicalTrials.gov, NCT02771938, and is closed to recruitment.
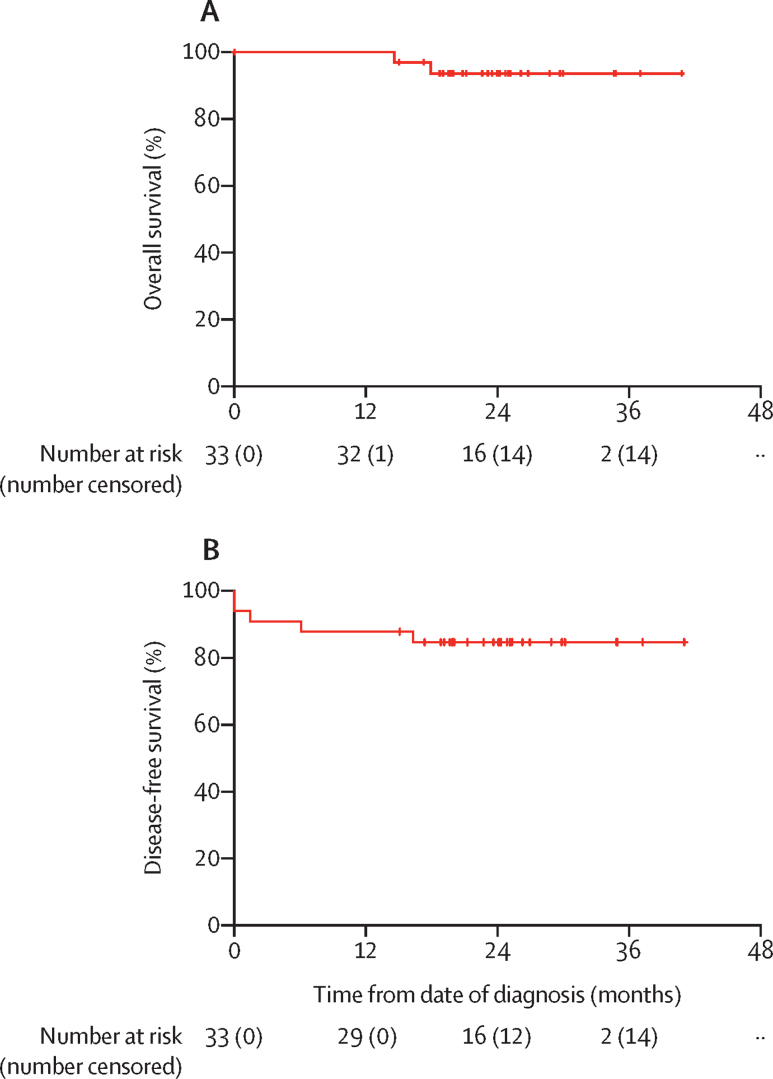
Findings: Between Jan 25, 2016, and Dec 11, 2017, 33 patients were enrolled. At 4 weeks after surgery, four (12·1%, 95% CI 3·4-28·2) of 33 patients had an open breast wound greater than 1 cm. One (3%) patient had confluent moist desquamation (grade 3). There were no serious treatment-related adverse events and no treatment-related deaths.
Interpretation: Preoperative radiotherapy followed by skin-sparing mastectomy and immediate DIEP flap reconstruction is feasible and technically safe, with rates of breast open wounds similar to those reported with post-mastectomy radiotherapy. A randomised trial comparing preoperative radiotherapy with post-mastectomy radiotherapy is required to precisely determine and compare surgical, oncological, and breast reconstruction outcomes, including quality of life.
Funding: Cancer Research UK, National Institute for Health Research.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
