Daniel J Van Hoving, Rulan Griesel, Graeme Meintjes, Yemisi Takwoingi, Gary Maartens, Eleanor A Ochodo
{"title":"Abdominal ultrasound for diagnosing abdominal tuberculosis or disseminated tuberculosis with abdominal involvement in HIV-positive individuals.","authors":"Daniel J Van Hoving, Rulan Griesel, Graeme Meintjes, Yemisi Takwoingi, Gary Maartens, Eleanor A Ochodo","doi":"10.1002/14651858.CD012777.pub2","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Accurate diagnosis of tuberculosis in people living with HIV is difficult. HIV-positive individuals have higher rates of extrapulmonary tuberculosis and the diagnosis of tuberculosis is often limited to imaging results. Ultrasound is such an imaging test that is widely used as a diagnostic tool (including point-of-care) in people suspected of having abdominal tuberculosis or disseminated tuberculosis with abdominal involvement.</p><p><strong>Objectives: </strong>To determine the diagnostic accuracy of abdominal ultrasound for detecting abdominal tuberculosis or disseminated tuberculosis with abdominal involvement in HIV-positive individuals.To investigate potential sources of heterogeneity in test accuracy, including clinical setting, ultrasound training level, and type of reference standard.</p><p><strong>Search methods: </strong>We searched for publications in any language up to 4 April 2019 in the following databases: MEDLINE, Embase, BIOSIS, Science Citation Index Expanded (SCI-EXPANDED), Social Sciences Citation Index (SSCI), Conference Proceedings Citation Index- Science (CPCI-S), and also ClinicalTrials.gov and the WHO International Clinical Trials Registry Platform to identify ongoing trials.</p><p><strong>Selection criteria: </strong>We included cross-sectional, cohort, and diagnostic case-control studies (prospective and retrospective) that compared the result of the index test (abdominal ultrasound) with one of the reference standards. We only included studies that allowed for extraction of numbers of true positives (TPs), true negatives (TNs), false positives (FPs), and false negatives (FNs). Participants were HIV-positive individuals aged 15 years and older. A higher-quality reference standard was the bacteriological confirmation of Mycobacterium tuberculosis from any clinical specimen, and a lower-quality reference standard was a clinical diagnosis of tuberculosis without microbiological confirmation. We excluded genitourinary tuberculosis.</p><p><strong>Data collection and analysis: </strong>For each study, two review authors independently extracted data using a standardized form. We assessed the quality of studies using a tailored Quality Assessment of Diagnostic Accuracy Studies-2 (QUADAS-2) tool. We used the bivariate model to estimate pooled sensitivity and specificity. When studies were few we simplified the bivariate model to separate univariate random-effects logistic regression models for sensitivity and specificity. We explored the influence of the type of reference standard on the accuracy estimates by conducting separate analyses for each type of reference standard. We assessed the certainty of the evidence using the GRADE approach.</p><p><strong>Main results: </strong>We included 11 studies. The risks of bias and concern about applicability were often high or unclear in all domains. We included six studies in the main analyses of any abnormal finding on abdominal ultrasound; five studies reported only individual lesions.The six studies of any abnormal finding were cross-sectional or cohort studies. Five of these (83%) were conducted in low- or middle-income countries, and one in a high-income country. The proportion of participants on antiretroviral therapy was none (1 study), fewer then 50% (4 studies), more than 50% (1 study), and not reported (5 studies). The first main analysis, studies using a higher-quality reference standard (bacteriological confirmation), had a pooled sensitivity of 63% (95% confidence interval (CI) 43% to 79%; 5 studies, 368 participants; very low-certainty evidence) and a pooled specificity of 68% (95% CI 42% to 87%; 5 studies, 511 participants; very low-certainty evidence). If the results were to be applied to a hypothetical cohort of 1000 people with HIV where 200 (20%) have tuberculosis then:- About 382 individuals would have an ultrasound result indicating tuberculosis; of these, 256 (67%) would be incorrectly classified as having tuberculosis (false positives).- Of the 618 individuals with a result indicating that tuberculosis is not present, 74 (12%) would be incorrectly classified as not having tuberculosis (false negatives).In the second main analysis involving studies using a lower-quality reference standard (clinical diagnosis), the pooled sensitivity was 68% (95% CI 45% to 85%; 4 studies, 195 participants; very low-certainty evidence) and the pooled specificity was 73% (95% CI 41% to 91%; 4 studies, 202 participants; very low-certainty evidence).</p><p><strong>Authors' conclusions: </strong>In HIV-positive individuals thought to have abdominal tuberculosis or disseminated tuberculosis with abdominal involvement, abdominal ultrasound appears to have 63% sensitivity and 68% specificity when tuberculosis was bacteriologically confirmed. These estimates are based on data that is limited, varied, and low-certainty.The low sensitivity of abdominal ultrasound means clinicians should not use a negative test result to rule out the disease, but rather consider the result in combination with other diagnostic strategies (including clinical signs, chest x-ray, lateral flow urine lipoarabinomannan assay (LF-LAM), and Xpert MTB/RIF). Research incorporating the test into tuberculosis diagnostic algorithms will help in delineating more precisely its value in diagnosing abdominal tuberculosis or disseminated tuberculosis with abdominal involvement.</p>","PeriodicalId":50709,"journal":{"name":"Central European Journal of Medicine","volume":"2 1","pages":"CD012777"},"PeriodicalIF":0.0000,"publicationDate":"2019-09-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6766789/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Central European Journal of Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1002/14651858.CD012777.pub2","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Accurate diagnosis of tuberculosis in people living with HIV is difficult. HIV-positive individuals have higher rates of extrapulmonary tuberculosis and the diagnosis of tuberculosis is often limited to imaging results. Ultrasound is such an imaging test that is widely used as a diagnostic tool (including point-of-care) in people suspected of having abdominal tuberculosis or disseminated tuberculosis with abdominal involvement.
Objectives: To determine the diagnostic accuracy of abdominal ultrasound for detecting abdominal tuberculosis or disseminated tuberculosis with abdominal involvement in HIV-positive individuals.To investigate potential sources of heterogeneity in test accuracy, including clinical setting, ultrasound training level, and type of reference standard.
Search methods: We searched for publications in any language up to 4 April 2019 in the following databases: MEDLINE, Embase, BIOSIS, Science Citation Index Expanded (SCI-EXPANDED), Social Sciences Citation Index (SSCI), Conference Proceedings Citation Index- Science (CPCI-S), and also ClinicalTrials.gov and the WHO International Clinical Trials Registry Platform to identify ongoing trials.
Selection criteria: We included cross-sectional, cohort, and diagnostic case-control studies (prospective and retrospective) that compared the result of the index test (abdominal ultrasound) with one of the reference standards. We only included studies that allowed for extraction of numbers of true positives (TPs), true negatives (TNs), false positives (FPs), and false negatives (FNs). Participants were HIV-positive individuals aged 15 years and older. A higher-quality reference standard was the bacteriological confirmation of Mycobacterium tuberculosis from any clinical specimen, and a lower-quality reference standard was a clinical diagnosis of tuberculosis without microbiological confirmation. We excluded genitourinary tuberculosis.
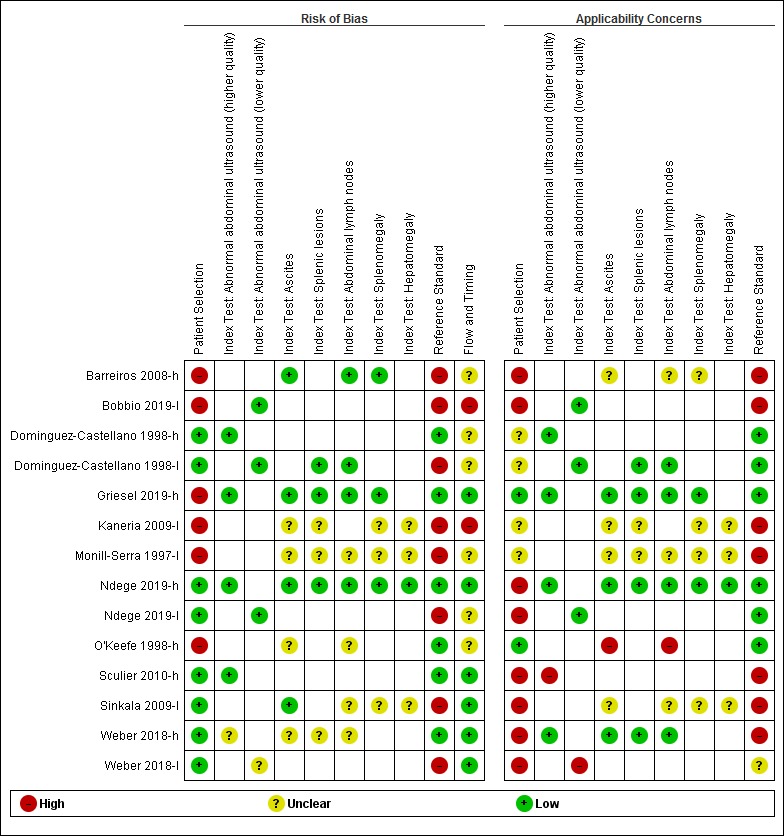
Data collection and analysis: For each study, two review authors independently extracted data using a standardized form. We assessed the quality of studies using a tailored Quality Assessment of Diagnostic Accuracy Studies-2 (QUADAS-2) tool. We used the bivariate model to estimate pooled sensitivity and specificity. When studies were few we simplified the bivariate model to separate univariate random-effects logistic regression models for sensitivity and specificity. We explored the influence of the type of reference standard on the accuracy estimates by conducting separate analyses for each type of reference standard. We assessed the certainty of the evidence using the GRADE approach.
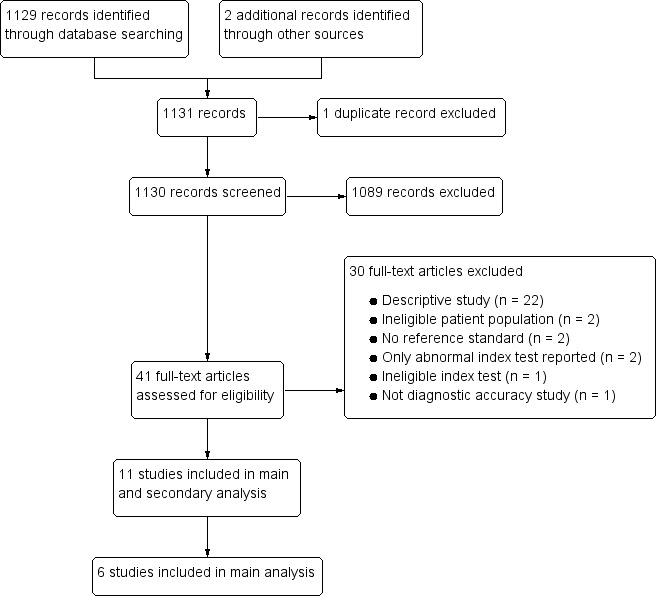
Main results: We included 11 studies. The risks of bias and concern about applicability were often high or unclear in all domains. We included six studies in the main analyses of any abnormal finding on abdominal ultrasound; five studies reported only individual lesions.The six studies of any abnormal finding were cross-sectional or cohort studies. Five of these (83%) were conducted in low- or middle-income countries, and one in a high-income country. The proportion of participants on antiretroviral therapy was none (1 study), fewer then 50% (4 studies), more than 50% (1 study), and not reported (5 studies). The first main analysis, studies using a higher-quality reference standard (bacteriological confirmation), had a pooled sensitivity of 63% (95% confidence interval (CI) 43% to 79%; 5 studies, 368 participants; very low-certainty evidence) and a pooled specificity of 68% (95% CI 42% to 87%; 5 studies, 511 participants; very low-certainty evidence). If the results were to be applied to a hypothetical cohort of 1000 people with HIV where 200 (20%) have tuberculosis then:- About 382 individuals would have an ultrasound result indicating tuberculosis; of these, 256 (67%) would be incorrectly classified as having tuberculosis (false positives).- Of the 618 individuals with a result indicating that tuberculosis is not present, 74 (12%) would be incorrectly classified as not having tuberculosis (false negatives).In the second main analysis involving studies using a lower-quality reference standard (clinical diagnosis), the pooled sensitivity was 68% (95% CI 45% to 85%; 4 studies, 195 participants; very low-certainty evidence) and the pooled specificity was 73% (95% CI 41% to 91%; 4 studies, 202 participants; very low-certainty evidence).
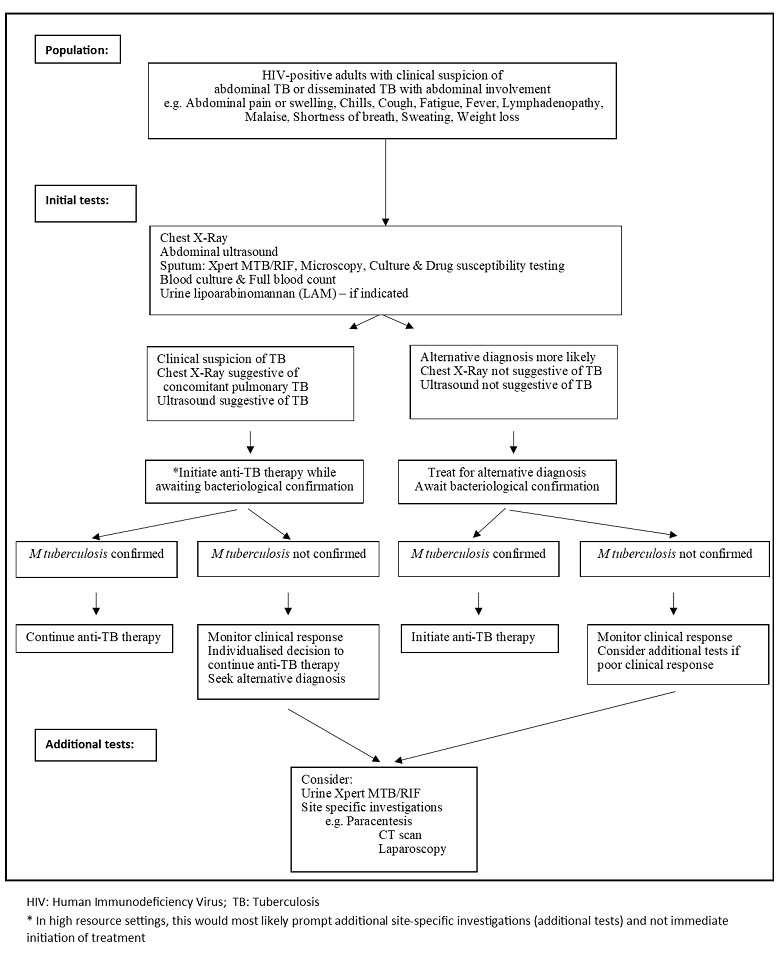
Authors' conclusions: In HIV-positive individuals thought to have abdominal tuberculosis or disseminated tuberculosis with abdominal involvement, abdominal ultrasound appears to have 63% sensitivity and 68% specificity when tuberculosis was bacteriologically confirmed. These estimates are based on data that is limited, varied, and low-certainty.The low sensitivity of abdominal ultrasound means clinicians should not use a negative test result to rule out the disease, but rather consider the result in combination with other diagnostic strategies (including clinical signs, chest x-ray, lateral flow urine lipoarabinomannan assay (LF-LAM), and Xpert MTB/RIF). Research incorporating the test into tuberculosis diagnostic algorithms will help in delineating more precisely its value in diagnosing abdominal tuberculosis or disseminated tuberculosis with abdominal involvement.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
