Roberto Stalla Alves da Fonseca, Viviane Martins Correa Boniatti, Michelle Carneiro Teixeira, Alessandra Preisig Werlang, Francielle Martins, Pedro Henrique Rigotti Soares, Leonardo da Silva Marques, Wagner Luis Nedel
{"title":"Mechanical Power in Prone Position Intubated Patients with COVID-19-Related ARDS: A Cohort Study.","authors":"Roberto Stalla Alves da Fonseca, Viviane Martins Correa Boniatti, Michelle Carneiro Teixeira, Alessandra Preisig Werlang, Francielle Martins, Pedro Henrique Rigotti Soares, Leonardo da Silva Marques, Wagner Luis Nedel","doi":"10.1155/2023/6604313","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Respiratory monitoring of mechanical ventilation (MV) is relevant and challenging in COVID-19. Mechanical power (MP) is a novel and promising monitoring tool in acute distress respiratory syndrome (ARDS), representing the amount of energy transferred from the ventilator to the patient. It encompasses several setting parameters and patient-dependent variables that could cause lung injury. MP can therefore be an additional tool in the assessment of these patients.</p><p><strong>Objective: </strong>This study aims to evaluate respiratory monitoring through MP and its relationship with mortality in patients with COVID-19-related ARDS (CARDS) under mechanical ventilation (MV) and prone position (PP) strategies.</p><p><strong>Methods: </strong>Retrospective, unicentric, and cohort studies. We included patients with CARDS under invasive MV and PP strategies. Information regarding MP, ventilation, and gas exchange was collected at 3 moments: (1) prior to the first PP, (2) during the first PP, and (3) during the last PP. We tested the relationship between MP and VR with in-hospital mortality.</p><p><strong>Results: </strong>We included 91 patients. There was a statistically significant difference in MP measurements between survivors and nonsurvivors only in the last prone position (<i>p</i> < 0.001). This is due to the significant increase in MP measurements in nonsurvivors (difference from the baseline: 3.63 J/min; 95% CI: 0.31 to 6.94), which was not observed in the group that survived (difference from the baseline: 0.02 J/min; 95% CI: -2.66 to 2.70). In multivariate analysis, MP (<i>p</i>=0.009) was associated with hospital death when corrected for confounder variables (SAPS 3 score, mechanical ventilation time, age, and number of prone sessions).</p><p><strong>Conclusions: </strong>MP is an independent predictor of mortality in PP patients with CARDS.</p>","PeriodicalId":46583,"journal":{"name":"Critical Care Research and Practice","volume":"2023 ","pages":"6604313"},"PeriodicalIF":1.8000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9995186/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Critical Care Research and Practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2023/6604313","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Respiratory monitoring of mechanical ventilation (MV) is relevant and challenging in COVID-19. Mechanical power (MP) is a novel and promising monitoring tool in acute distress respiratory syndrome (ARDS), representing the amount of energy transferred from the ventilator to the patient. It encompasses several setting parameters and patient-dependent variables that could cause lung injury. MP can therefore be an additional tool in the assessment of these patients.
Objective: This study aims to evaluate respiratory monitoring through MP and its relationship with mortality in patients with COVID-19-related ARDS (CARDS) under mechanical ventilation (MV) and prone position (PP) strategies.
Methods: Retrospective, unicentric, and cohort studies. We included patients with CARDS under invasive MV and PP strategies. Information regarding MP, ventilation, and gas exchange was collected at 3 moments: (1) prior to the first PP, (2) during the first PP, and (3) during the last PP. We tested the relationship between MP and VR with in-hospital mortality.
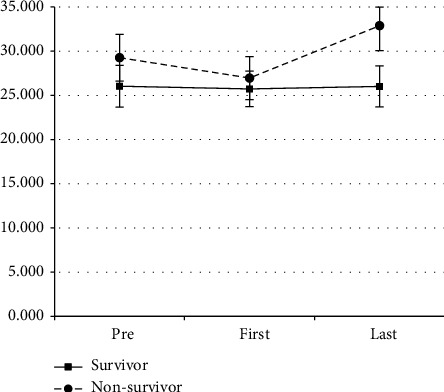
Results: We included 91 patients. There was a statistically significant difference in MP measurements between survivors and nonsurvivors only in the last prone position (p < 0.001). This is due to the significant increase in MP measurements in nonsurvivors (difference from the baseline: 3.63 J/min; 95% CI: 0.31 to 6.94), which was not observed in the group that survived (difference from the baseline: 0.02 J/min; 95% CI: -2.66 to 2.70). In multivariate analysis, MP (p=0.009) was associated with hospital death when corrected for confounder variables (SAPS 3 score, mechanical ventilation time, age, and number of prone sessions).
Conclusions: MP is an independent predictor of mortality in PP patients with CARDS.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
