Italian Real-World Analysis of the Impact of Polypharmacy and Aging on the Risk of Multiple Drug-Drug Interactions (DDIs) in HCV Patients Treated with Pangenotypic Direct-Acting Antivirals (pDAA).
{"title":"Italian Real-World Analysis of the Impact of Polypharmacy and Aging on the Risk of Multiple Drug-Drug Interactions (DDIs) in HCV Patients Treated with Pangenotypic Direct-Acting Antivirals (pDAA).","authors":"Stefano Fagiuoli, Pierluigi Toniutto, Nicola Coppola, Domenica Daniela Ancona, Margherita Andretta, Fausto Bartolini, Fulvio Ferrante, Alessandro Lupi, Stefano Palcic, Francesca Vittoria Rizzi, Davide Re, Gema Alvarez Nieto, Candido Hernandez, Francesca Frigerio, Valentina Perrone, Luca Degli Esposti, Alessandra Mangia","doi":"10.2147/TCRM.S394467","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>The study aims at investigating the impact of polymedication and aging in the prevalence of multiple drug-drug interactions (DDIs) on HCV patients treated with sofosbuvir/velpatasvir (SOF/VEL) or glecaprevir/pibrentasvir (GLE/PIB).</p><p><strong>Patients and methods: </strong>This is a retrospective analysis based on administrative data covering around 6.9 million individuals. Patients treated with SOF/VEL or GLE/PIB over November 2017-March 2020 were included. Index date corresponded to SOF/VEL or GLE/PIB first prescription during such period; patients were followed up for treatment duration. Analyses were then focused on patients with ≥2 comedications at risk of multiple DDIs. The severity and the effect of multiple DDI were identified using the Liverpool University tool.</p><p><strong>Results: </strong>A total of 2057 patients with SOF/VEL and 2128 with GLE/PIB were selected. Mean age of SOF/VEL patients was 58.5 years, higher than GLE/PIB ones (52.5 years) (p < 0.001), and patients >50 years were more present in SOF/VEL vs GLE/PIB cohorts: 72% vs 58%, (p < 0.001). Most prescribed co-medications were cardiovascular, alimentary and nervous system drugs. Proportion of patients with ≥2 comedications was higher in SOF/VEL compared to GLE/PIB cohort (56.5% vs 32.3%, p < 0.001). Those at high-risk of multiple DDIs accounted for 11.6% (N = 135) of SOF/VEL and 19.6% (N = 135) of GLE/PIB (p < 0.001) patients with ≥2 comedications. Among them, the potential effect of DDI was a decrease of DAA serum levels (11% of SOF/VEL and GLE/PIB patients) and an increased concentration of comedication serum levels (14% of SOF/VEL and 42% of GLE/PIB patients).</p><p><strong>Conclusion: </strong>This real-world analysis provided a thorough characterization on the burden of polymedication regimens in HCV patients treated with SOF/VEL or GLE/PIB that expose such patients to an increased risk of DDIs. In our sample population, SOF/VEL regimen was more frequently detected on elderly patients and on those with ≥2 comedications at risk of multi-DDI, ie, among patients characterized by higher rates of comorbidities and polypharmacy.</p>","PeriodicalId":48769,"journal":{"name":"Therapeutics and Clinical Risk Management","volume":"19 ","pages":"57-65"},"PeriodicalIF":2.3000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/a2/87/tcrm-19-57.PMC9868280.pdf","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Therapeutics and Clinical Risk Management","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.2147/TCRM.S394467","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
引用次数: 1
Abstract
Purpose: The study aims at investigating the impact of polymedication and aging in the prevalence of multiple drug-drug interactions (DDIs) on HCV patients treated with sofosbuvir/velpatasvir (SOF/VEL) or glecaprevir/pibrentasvir (GLE/PIB).
Patients and methods: This is a retrospective analysis based on administrative data covering around 6.9 million individuals. Patients treated with SOF/VEL or GLE/PIB over November 2017-March 2020 were included. Index date corresponded to SOF/VEL or GLE/PIB first prescription during such period; patients were followed up for treatment duration. Analyses were then focused on patients with ≥2 comedications at risk of multiple DDIs. The severity and the effect of multiple DDI were identified using the Liverpool University tool.
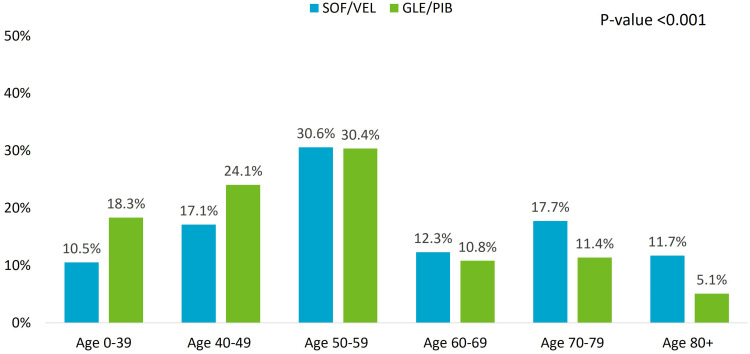
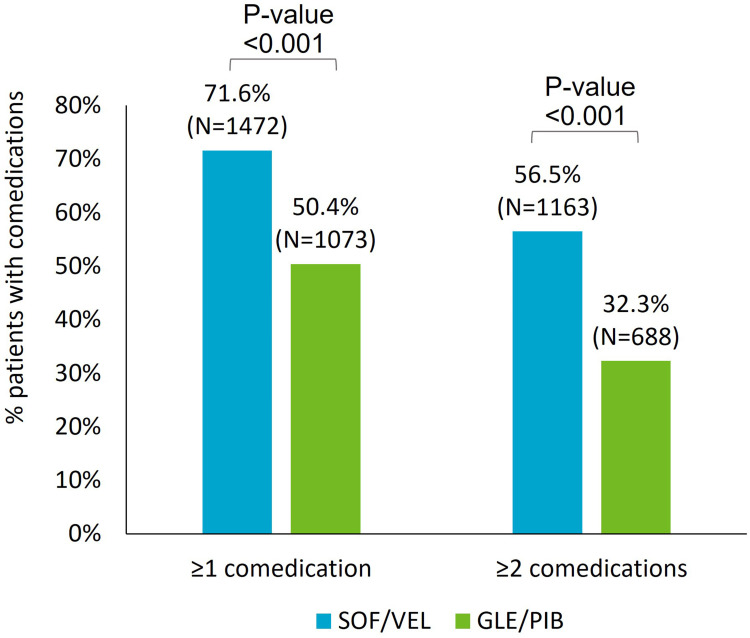
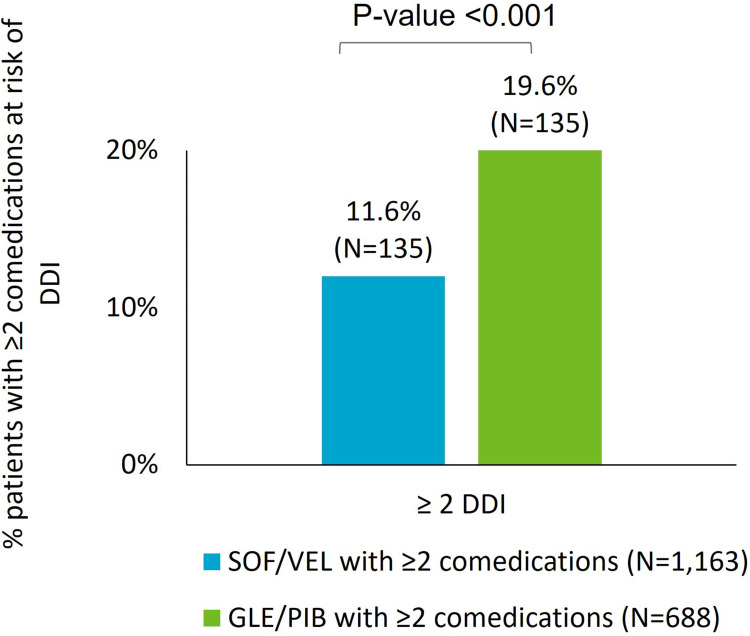
Results: A total of 2057 patients with SOF/VEL and 2128 with GLE/PIB were selected. Mean age of SOF/VEL patients was 58.5 years, higher than GLE/PIB ones (52.5 years) (p < 0.001), and patients >50 years were more present in SOF/VEL vs GLE/PIB cohorts: 72% vs 58%, (p < 0.001). Most prescribed co-medications were cardiovascular, alimentary and nervous system drugs. Proportion of patients with ≥2 comedications was higher in SOF/VEL compared to GLE/PIB cohort (56.5% vs 32.3%, p < 0.001). Those at high-risk of multiple DDIs accounted for 11.6% (N = 135) of SOF/VEL and 19.6% (N = 135) of GLE/PIB (p < 0.001) patients with ≥2 comedications. Among them, the potential effect of DDI was a decrease of DAA serum levels (11% of SOF/VEL and GLE/PIB patients) and an increased concentration of comedication serum levels (14% of SOF/VEL and 42% of GLE/PIB patients).
Conclusion: This real-world analysis provided a thorough characterization on the burden of polymedication regimens in HCV patients treated with SOF/VEL or GLE/PIB that expose such patients to an increased risk of DDIs. In our sample population, SOF/VEL regimen was more frequently detected on elderly patients and on those with ≥2 comedications at risk of multi-DDI, ie, among patients characterized by higher rates of comorbidities and polypharmacy.
期刊介绍:
Therapeutics and Clinical Risk Management is an international, peer-reviewed journal of clinical therapeutics and risk management, focusing on concise rapid reporting of clinical studies in all therapeutic areas, outcomes, safety, and programs for the effective, safe, and sustained use of medicines, therapeutic and surgical interventions in all clinical areas.
The journal welcomes submissions covering original research, clinical and epidemiological studies, reviews, guidelines, expert opinion and commentary. The journal will consider case reports but only if they make a valuable and original contribution to the literature.
As of 18th March 2019, Therapeutics and Clinical Risk Management will no longer consider meta-analyses for publication.
The journal does not accept study protocols, animal-based or cell line-based studies.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
