Ping-Chen Hou, Nathalie Del Agua, Su M Lwin, Chao-Kai Hsu, John A McGrath
{"title":"Innovations in the Treatment of Dystrophic Epidermolysis Bullosa (DEB): Current Landscape and Prospects.","authors":"Ping-Chen Hou, Nathalie Del Agua, Su M Lwin, Chao-Kai Hsu, John A McGrath","doi":"10.2147/TCRM.S386923","DOIUrl":null,"url":null,"abstract":"<p><p>Dystrophic epidermolysis bullosa (DEB) is one of the major types of EB, a rare hereditary group of trauma-induced blistering skin disorders. DEB is caused by inherited pathogenic variants in the <i>COL7A1</i> gene, which encodes type VII collagen, the major component of anchoring fibrils which maintain adhesion between the outer epidermis and underlying dermis. DEB can be subclassified into dominant (DDEB) and recessive (RDEB) forms. Generally, DDEB has a milder phenotype, while RDEB patients often have more extensive blistering, chronic inflammation, skin fibrosis, and a propensity for squamous cell carcinoma development, collectively impacting on daily activities and life expectancy. At present, best practice treatments are mostly supportive, and thus there is a considerable burden of disease with unmet therapeutic need. Over the last 20 years, considerable translational research efforts have focused on either trying to cure DEB by direct correction of the <i>COL7A1</i> gene pathology, or by modifying secondary inflammation to lessen phenotypic severity and improve patient symptoms such as poor wound healing, itch, and pain. In this review, we provide an overview and update on various therapeutic innovations for DEB, including gene therapy, cell-based therapy, protein therapy, and disease-modifying and symptomatic control agents. We outline the progress and challenges for each treatment modality and identify likely prospects for future clinical impact.</p>","PeriodicalId":48769,"journal":{"name":"Therapeutics and Clinical Risk Management","volume":"19 ","pages":"455-473"},"PeriodicalIF":2.3000,"publicationDate":"2023-06-14","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/d2/0a/tcrm-19-455.PMC10277004.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Therapeutics and Clinical Risk Management","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.2147/TCRM.S386923","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
引用次数: 0
Abstract
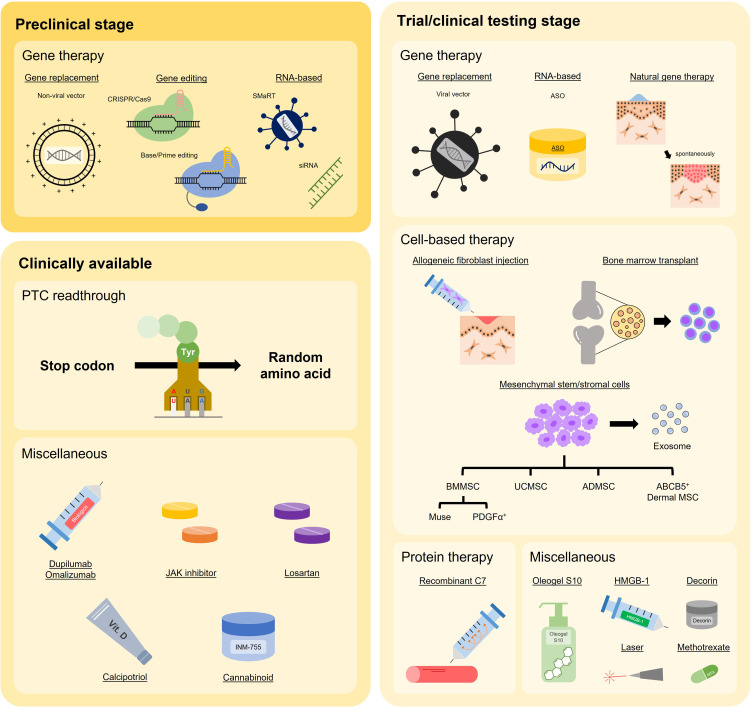
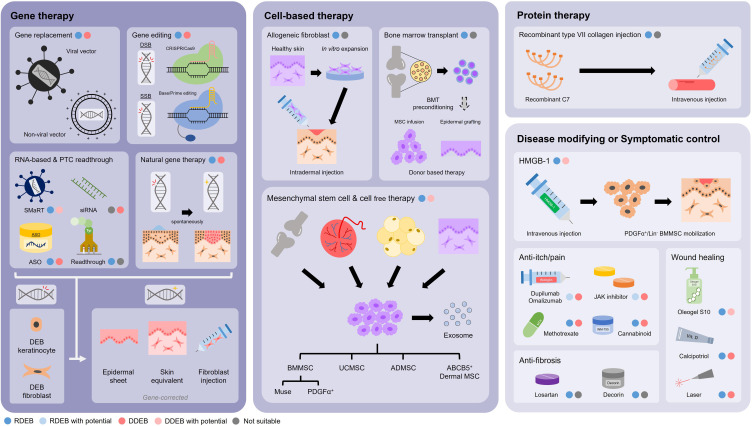
Dystrophic epidermolysis bullosa (DEB) is one of the major types of EB, a rare hereditary group of trauma-induced blistering skin disorders. DEB is caused by inherited pathogenic variants in the COL7A1 gene, which encodes type VII collagen, the major component of anchoring fibrils which maintain adhesion between the outer epidermis and underlying dermis. DEB can be subclassified into dominant (DDEB) and recessive (RDEB) forms. Generally, DDEB has a milder phenotype, while RDEB patients often have more extensive blistering, chronic inflammation, skin fibrosis, and a propensity for squamous cell carcinoma development, collectively impacting on daily activities and life expectancy. At present, best practice treatments are mostly supportive, and thus there is a considerable burden of disease with unmet therapeutic need. Over the last 20 years, considerable translational research efforts have focused on either trying to cure DEB by direct correction of the COL7A1 gene pathology, or by modifying secondary inflammation to lessen phenotypic severity and improve patient symptoms such as poor wound healing, itch, and pain. In this review, we provide an overview and update on various therapeutic innovations for DEB, including gene therapy, cell-based therapy, protein therapy, and disease-modifying and symptomatic control agents. We outline the progress and challenges for each treatment modality and identify likely prospects for future clinical impact.
萎缩性表皮松解症(DEB)是EB的主要类型之一,是一种罕见的遗传性外伤诱发的大疱性皮肤病。DEB 是由 COL7A1 基因的遗传致病变体引起的,该基因编码 VII 型胶原蛋白,而 VII 型胶原蛋白是锚定纤维的主要成分,可维持表皮层和真皮层之间的粘附力。DEB 可分为显性(DDEB)和隐性(RDEB)两种。一般来说,显性遗传性 DEB 的表型较轻,而隐性遗传性 DEB 患者通常会出现更广泛的水疱、慢性炎症、皮肤纤维化以及鳞状细胞癌的发展倾向,这些都会影响患者的日常活动和预期寿命。目前,最佳治疗方法大多是支持性的,因此,有相当大的疾病负担和治疗需求尚未得到满足。在过去的 20 年中,大量转化研究工作集中在试图通过直接纠正 COL7A1 基因病理学来治愈 DEB,或通过改变继发性炎症来减轻表型的严重程度并改善患者症状,如伤口愈合不良、瘙痒和疼痛。在这篇综述中,我们概述了针对 DEB 的各种创新疗法,包括基因疗法、细胞疗法、蛋白质疗法以及疾病修饰和症状控制药物。我们概述了每种治疗方法所取得的进展和面临的挑战,并确定了未来临床影响的可能前景。
期刊介绍:
Therapeutics and Clinical Risk Management is an international, peer-reviewed journal of clinical therapeutics and risk management, focusing on concise rapid reporting of clinical studies in all therapeutic areas, outcomes, safety, and programs for the effective, safe, and sustained use of medicines, therapeutic and surgical interventions in all clinical areas.
The journal welcomes submissions covering original research, clinical and epidemiological studies, reviews, guidelines, expert opinion and commentary. The journal will consider case reports but only if they make a valuable and original contribution to the literature.
As of 18th March 2019, Therapeutics and Clinical Risk Management will no longer consider meta-analyses for publication.
The journal does not accept study protocols, animal-based or cell line-based studies.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
