Dong Wang, Lei Deng, Ruipeng Zhang, Yiyue Zhou, Jun Zeng, Hua Jiang
{"title":"Efficacy of intraosseous access for trauma resuscitation: a systematic review and meta-analysis.","authors":"Dong Wang, Lei Deng, Ruipeng Zhang, Yiyue Zhou, Jun Zeng, Hua Jiang","doi":"10.1186/s13017-023-00487-7","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>During medical emergencies, intraosseous (IO) access and intravenous (IV) access are methods of administering therapies and medications to patients. Treating patients in emergency medical situations is a highly time sensitive practice; however, research into the optimal access method is limited and existing systematic reviews have only considered out-of-hospital cardiac arrest (OHCA) patients. We focused on severe trauma patients and conducted a systematic review to evaluate the efficacy and efficiency of intraosseous (IO) access compared to intravenous (IV) access for trauma resuscitation in prehospital care.</p><p><strong>Materials and method: </strong>PubMed, Web of Science, Cochrane Library, EMBASE, ScienceDirect, banque de données en santé publique and CNKI databases were searched for articles published between January 1, 2000, and January 31, 2023. Adult trauma patients were included, regardless of race, nationality, and region. OHCA patients and other types of patients were excluded. The experimental and control groups received IO and IV access, respectively, in the pre-hospital and emergency departments for salvage. The primary outcome was success rate on first attempt, which was defined as secure needle position in the marrow cavity or a peripheral vein, with normal fluid flow. Secondary outcomes included mean time to resuscitation, mean procedure time, and complications.</p><p><strong>Results: </strong>Three reviewers independently screened the literature, extracted the data, and assessed the risk of bias in the included studies; meta-analyses were then performed using Review Manager (Version 5.4; Cochrane, Oxford, UK). The success rate on first attempt was significant higher for IO access than for IV access (RR = 1.46, 95% CI [1.16, 1.85], P = 0.001). The mean procedure time was significantly reduced (MD = - 5.67, 95% CI [- 9.26, - 2.07], P = 0.002). There was no significant difference in mean time to resuscitation (MD = - 1.00, 95% CI [- 3.18, 1.17], P = 0.37) and complications (RR = 1.22, 95% CI [0.14, 10.62], P = 0.86) between the IO and IV groups.</p><p><strong>Conclusion: </strong>The success rate on first attempt of IO access was much higher than that of IV access for trauma patients, and the mean procedure time of IO access was significantly less when compared to IV access. Therefore, IO access should be suggested as an urgent vascular access for hypotensive trauma patients, especially those who are under severe shock.</p>","PeriodicalId":48867,"journal":{"name":"World Journal of Emergency Surgery","volume":"18 1","pages":"17"},"PeriodicalIF":5.8000,"publicationDate":"2023-03-14","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10012735/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"World Journal of Emergency Surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s13017-023-00487-7","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"EMERGENCY MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
Background: During medical emergencies, intraosseous (IO) access and intravenous (IV) access are methods of administering therapies and medications to patients. Treating patients in emergency medical situations is a highly time sensitive practice; however, research into the optimal access method is limited and existing systematic reviews have only considered out-of-hospital cardiac arrest (OHCA) patients. We focused on severe trauma patients and conducted a systematic review to evaluate the efficacy and efficiency of intraosseous (IO) access compared to intravenous (IV) access for trauma resuscitation in prehospital care.
Materials and method: PubMed, Web of Science, Cochrane Library, EMBASE, ScienceDirect, banque de données en santé publique and CNKI databases were searched for articles published between January 1, 2000, and January 31, 2023. Adult trauma patients were included, regardless of race, nationality, and region. OHCA patients and other types of patients were excluded. The experimental and control groups received IO and IV access, respectively, in the pre-hospital and emergency departments for salvage. The primary outcome was success rate on first attempt, which was defined as secure needle position in the marrow cavity or a peripheral vein, with normal fluid flow. Secondary outcomes included mean time to resuscitation, mean procedure time, and complications.
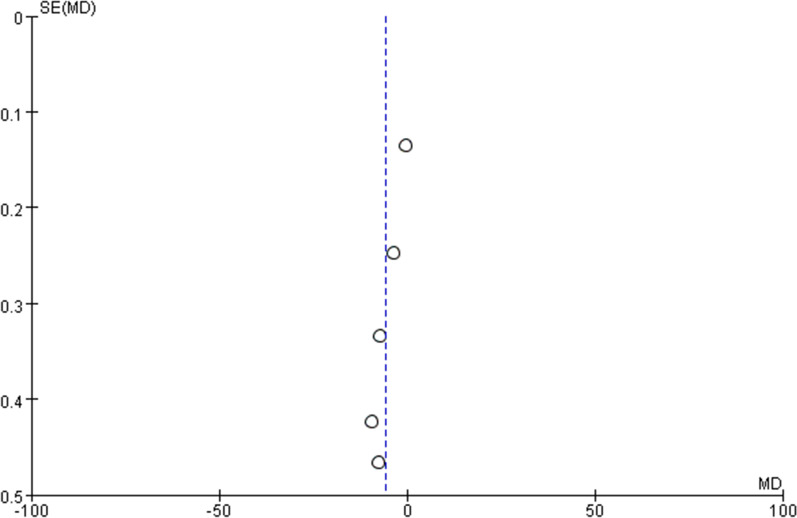
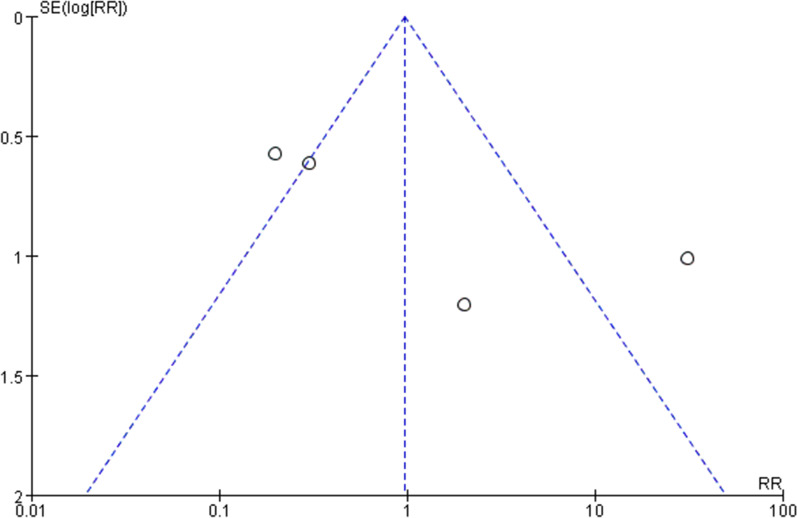
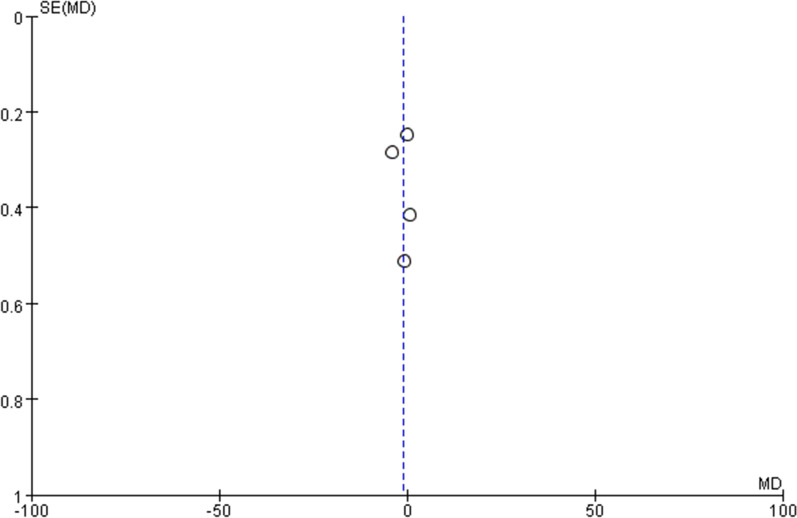
Results: Three reviewers independently screened the literature, extracted the data, and assessed the risk of bias in the included studies; meta-analyses were then performed using Review Manager (Version 5.4; Cochrane, Oxford, UK). The success rate on first attempt was significant higher for IO access than for IV access (RR = 1.46, 95% CI [1.16, 1.85], P = 0.001). The mean procedure time was significantly reduced (MD = - 5.67, 95% CI [- 9.26, - 2.07], P = 0.002). There was no significant difference in mean time to resuscitation (MD = - 1.00, 95% CI [- 3.18, 1.17], P = 0.37) and complications (RR = 1.22, 95% CI [0.14, 10.62], P = 0.86) between the IO and IV groups.
Conclusion: The success rate on first attempt of IO access was much higher than that of IV access for trauma patients, and the mean procedure time of IO access was significantly less when compared to IV access. Therefore, IO access should be suggested as an urgent vascular access for hypotensive trauma patients, especially those who are under severe shock.
背景:在医疗紧急情况下,骨内(IO)通道和静脉(IV)通道是给患者提供治疗和药物的方法。在紧急医疗情况下治疗患者是一种高度时间敏感的做法;然而,对最佳获取方法的研究是有限的,现有的系统评价只考虑院外心脏骤停(OHCA)患者。我们以严重创伤患者为研究对象,对院前创伤复苏中骨内(IO)通路与静脉(IV)通路的疗效和效率进行了系统评价。材料和方法:检索2000年1月1日至2023年1月31日期间发表的文章,检索PubMed、Web of Science、Cochrane Library、EMBASE、ScienceDirect、banque de donnsames en sant publicque和CNKI数据库。纳入成人创伤患者,不分种族、国籍和地区。排除OHCA患者及其他类型患者。实验组和对照组分别在院前和急诊科进行IO和IV通路抢救。主要结果是第一次尝试的成功率,其定义为针头在骨髓腔或外周静脉中的安全位置,液体流动正常。次要结局包括平均复苏时间、平均手术时间和并发症。结果:三位审稿人独立筛选文献,提取资料,并评估纳入研究的偏倚风险;然后使用Review Manager (Version 5.4;科克伦,牛津,英国)。首次尝试的成功率明显高于静脉输注(RR = 1.46, 95% CI [1.16, 1.85], P = 0.001)。平均手术时间显著缩短(MD = - 5.67, 95% CI [- 9.26, - 2.07], P = 0.002)。两组患者平均复苏时间(MD = - 1.00, 95% CI [- 3.18, 1.17], P = 0.37)和并发症(RR = 1.22, 95% CI [0.14, 10.62], P = 0.86)差异无统计学意义。结论:创伤患者首次入路成功率明显高于静脉入路,且平均手术时间明显少于静脉入路。因此,对于低血压创伤患者,特别是严重休克患者,应建议将IO通路作为紧急血管通路。
期刊介绍:
The World Journal of Emergency Surgery is an open access, peer-reviewed journal covering all facets of clinical and basic research in traumatic and non-traumatic emergency surgery and related fields. Topics include emergency surgery, acute care surgery, trauma surgery, intensive care, trauma management, and resuscitation, among others.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
