{"title":"Characterization of Favorable Right Ventricular Dimensions for Optimal Reverse Remodeling Following Pulmonary Valve Replacement","authors":"","doi":"10.1053/j.semtcvs.2022.11.014","DOIUrl":null,"url":null,"abstract":"<div><p><span><span>We sought to couple current cardiac magnetic resonance<span> (CMR) thresholds of right ventricular (RV) size and function with longitudinal trajectories of RV recovery, after pulmonary valve replacement (PVR). We aimed to identify optimal timing of PVR and couple CMR-based metrics with contemporaneous echocardiographic metrics. From June 2002 to January 2019, 174 patients with severe </span></span>pulmonary regurgitation<span><span><span> and peak RV outflow tract gradient <30 mm Hg underwent PVR at Cleveland Clinic. Mean age was 35 ± 16 years and 60 (34%) had concomitant </span>tricuspid valve<span> surgery. RV end diastolic area index (RVEDAi) and function metrics were measured by offline image review on preoperative and 794 postoperative echocardiograms. Contemporaneous RV </span></span>end diastolic volume index (RVEDVi) was assessed on CMR and correlated to RVEDAi. Multiphase nonlinear mixed-effects models were used to analyze the longitudinal change in RV size and function after PVR. RVEDAi was correlated with RVEDVi (</span></span><em>P</em> < 0.0001, r = 0.59). RVEDAi decreased slowly over 10 years following PVR. An inflection point at 24 cm<sup>2</sup>/m<sup>2</sup> was noted at 1 year post-PVR and was associated with failure of RV reverse remodeling and RVEDVi ≥150 mL/m<sup>2</sup>. Compared to patients with preoperative RVEDVi ≥150 mL/m<sup>2</sup>, patients with RVEDVi <150 mL/m<sup>2</sup> had accelerated recovery of longitudinal trajectories of RV size and function metrics on echocardiograms. Reverse remodeling of RV following PVR is an ongoing process. Current accepted threshold values for PVR are associated with greatest RV recovery, suggesting that earlier PVR is warranted. Echocardiography can potentially be utilized in lieu of CMR for surveillance and interventional triage.</p></div>","PeriodicalId":48592,"journal":{"name":"Seminars in Thoracic and Cardiovascular Surgery","volume":"36 3","pages":"Pages 345-355"},"PeriodicalIF":2.5000,"publicationDate":"2024-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Seminars in Thoracic and Cardiovascular Surgery","FirstCategoryId":"3","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S1043067923000333","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/2/24 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
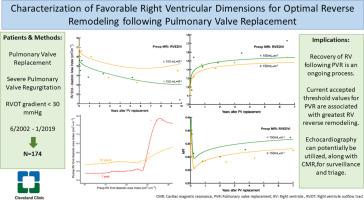
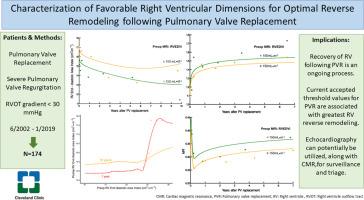
We sought to couple current cardiac magnetic resonance (CMR) thresholds of right ventricular (RV) size and function with longitudinal trajectories of RV recovery, after pulmonary valve replacement (PVR). We aimed to identify optimal timing of PVR and couple CMR-based metrics with contemporaneous echocardiographic metrics. From June 2002 to January 2019, 174 patients with severe pulmonary regurgitation and peak RV outflow tract gradient <30 mm Hg underwent PVR at Cleveland Clinic. Mean age was 35 ± 16 years and 60 (34%) had concomitant tricuspid valve surgery. RV end diastolic area index (RVEDAi) and function metrics were measured by offline image review on preoperative and 794 postoperative echocardiograms. Contemporaneous RV end diastolic volume index (RVEDVi) was assessed on CMR and correlated to RVEDAi. Multiphase nonlinear mixed-effects models were used to analyze the longitudinal change in RV size and function after PVR. RVEDAi was correlated with RVEDVi (P < 0.0001, r = 0.59). RVEDAi decreased slowly over 10 years following PVR. An inflection point at 24 cm2/m2 was noted at 1 year post-PVR and was associated with failure of RV reverse remodeling and RVEDVi ≥150 mL/m2. Compared to patients with preoperative RVEDVi ≥150 mL/m2, patients with RVEDVi <150 mL/m2 had accelerated recovery of longitudinal trajectories of RV size and function metrics on echocardiograms. Reverse remodeling of RV following PVR is an ongoing process. Current accepted threshold values for PVR are associated with greatest RV recovery, suggesting that earlier PVR is warranted. Echocardiography can potentially be utilized in lieu of CMR for surveillance and interventional triage.
期刊介绍:
Seminars in Thoracic and Cardiovascular Surgery is devoted to providing a forum for cardiothoracic surgeons to disseminate and discuss important new information and to gain insight into unresolved areas of question in the specialty. Each issue presents readers with a selection of original peer-reviewed articles accompanied by editorial commentary from specialists in the field. In addition, readers are offered valuable invited articles: State of Views editorials and Current Readings highlighting the latest contributions on central or controversial issues. Another prized feature is expert roundtable discussions in which experts debate critical questions for cardiothoracic treatment and care. Seminars is an invitation-only publication that receives original submissions transferred ONLY from its sister publication, The Journal of Thoracic and Cardiovascular Surgery. As we continue to expand the reach of the Journal, we will explore the possibility of accepting unsolicited manuscripts in the future.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
