Extended dual antiplatelet therapy following percutaneous coronary intervention in clinically important patient subgroups: a systematic review and meta-analysis.
Jesse Elliott, Shannon E Kelly, Zemin Bai, Becky Skidmore, Michel Boucher, Derek So, George A Wells
{"title":"Extended dual antiplatelet therapy following percutaneous coronary intervention in clinically important patient subgroups: a systematic review and meta-analysis.","authors":"Jesse Elliott, Shannon E Kelly, Zemin Bai, Becky Skidmore, Michel Boucher, Derek So, George A Wells","doi":"10.9778/cmajo.20210119","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Dual antiplatelet therapy (DAPT) is routinely given to patients after percutaneous coronary intervention (PCI) with stenting; however, optimal duration remains uncertain in some situations. We assessed the benefits and harms of extending DAPT beyond 1 year after PCI in clinically important patient subgroups.</p><p><strong>Methods: </strong>We conducted a systematic review and meta-analysis. We searched electronic databases (Embase, MEDLINE, PubMed, Cochrane Library) and grey literature (from inception to Nov. 5, 2021) and included randomized controlled trials (RCTs) of extended DAPT (> 12 mo) compared with DAPT for 6-12 months following PCI with stenting. The primary outcome was death (all cause, cardiovascular, noncardiovascular); secondary outcomes included major adverse cardiovascular and cerebrovascular events, myocardial infarction (MI), stroke, stent thrombosis and bleeding. Subgroups were based on prespecified patient characteristics (prior MI, acute coronary syndrome [ACS], diabetes mellitus, age, smoking status). Data were analyzed by random-effects pairwise meta-analysis.</p><p><strong>Results: </strong>We identified 9 RCTs that provided subgroup data. We found that extended DAPT reduced the risk of MI and stent thrombosis but increased the risk of bleeding, compared with standard DAPT, with no difference in the risk of all-cause death (relative risk [RR] 1.07, 95% confidence interval [CI] 0.80-1.42) or cardiovascular death (RR 0.98, 95% CI 0.74-1.30). We found that patients with a prior MI, with ACS at presentation, without diabetes or aged younger than 75 years may derive the most benefit from extended DAPT. Among patients who received extended DAPT, the risk of all-cause death was significantly increased among those with no prior MI (RR 1.64, 95% CI 1.08-2.24), whereas there was no significant difference in the risk of all-cause death between standard and extended DAPT for patients with ACS (RR 1.20, 95% CI 0.51-2.83), with diabetes (RR 1.27, 95% CI 0.86-1.89), aged older than 75 years (RR 1.32, 95% CI 0.39-4.54) or who smoked (RR 0.90, 95% CI 0.42-1.92). Similar results were found for cardiovascular death, where data were available.</p><p><strong>Interpretation: </strong>Patients with a previous MI with ACS at presentation, without diabetes, or aged younger than 75 years may derive the most benefit from extended DAPT. These findings support the need for careful selection of patients who may benefit most from extended DAPT.</p><p><strong>Study registration: </strong>PROSPERO no. CRD42018082587.</p>","PeriodicalId":10432,"journal":{"name":"CMAJ open","volume":"11 1","pages":"E118-E130"},"PeriodicalIF":0.0000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/f9/e1/cmajo.20210119.PMC9911127.pdf","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"CMAJ open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.9778/cmajo.20210119","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 1
Abstract
Background: Dual antiplatelet therapy (DAPT) is routinely given to patients after percutaneous coronary intervention (PCI) with stenting; however, optimal duration remains uncertain in some situations. We assessed the benefits and harms of extending DAPT beyond 1 year after PCI in clinically important patient subgroups.
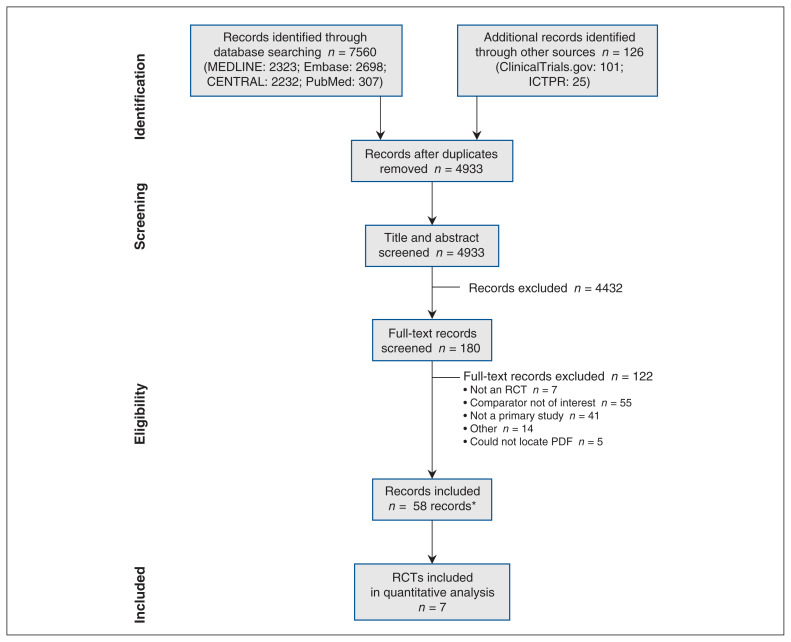
Methods: We conducted a systematic review and meta-analysis. We searched electronic databases (Embase, MEDLINE, PubMed, Cochrane Library) and grey literature (from inception to Nov. 5, 2021) and included randomized controlled trials (RCTs) of extended DAPT (> 12 mo) compared with DAPT for 6-12 months following PCI with stenting. The primary outcome was death (all cause, cardiovascular, noncardiovascular); secondary outcomes included major adverse cardiovascular and cerebrovascular events, myocardial infarction (MI), stroke, stent thrombosis and bleeding. Subgroups were based on prespecified patient characteristics (prior MI, acute coronary syndrome [ACS], diabetes mellitus, age, smoking status). Data were analyzed by random-effects pairwise meta-analysis.
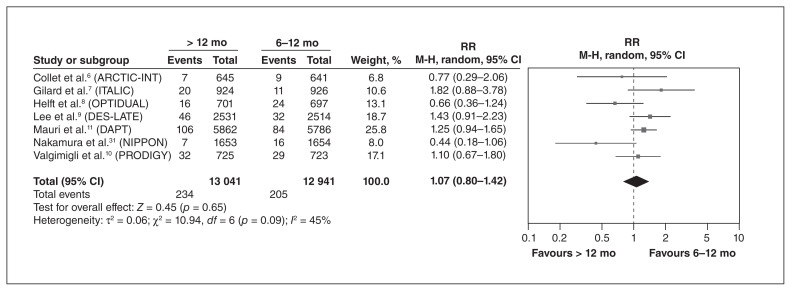
Results: We identified 9 RCTs that provided subgroup data. We found that extended DAPT reduced the risk of MI and stent thrombosis but increased the risk of bleeding, compared with standard DAPT, with no difference in the risk of all-cause death (relative risk [RR] 1.07, 95% confidence interval [CI] 0.80-1.42) or cardiovascular death (RR 0.98, 95% CI 0.74-1.30). We found that patients with a prior MI, with ACS at presentation, without diabetes or aged younger than 75 years may derive the most benefit from extended DAPT. Among patients who received extended DAPT, the risk of all-cause death was significantly increased among those with no prior MI (RR 1.64, 95% CI 1.08-2.24), whereas there was no significant difference in the risk of all-cause death between standard and extended DAPT for patients with ACS (RR 1.20, 95% CI 0.51-2.83), with diabetes (RR 1.27, 95% CI 0.86-1.89), aged older than 75 years (RR 1.32, 95% CI 0.39-4.54) or who smoked (RR 0.90, 95% CI 0.42-1.92). Similar results were found for cardiovascular death, where data were available.
Interpretation: Patients with a previous MI with ACS at presentation, without diabetes, or aged younger than 75 years may derive the most benefit from extended DAPT. These findings support the need for careful selection of patients who may benefit most from extended DAPT.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
