Identifying clusters of coexisting conditions and outcomes among adults admitted to hospital with community-acquired pneumonia: a multicentre cohort study.
Sarah L Malecki, Hae Young Jung, Anne Loffler, Mark A Green, Samir Gupta, Derek MacFadden, Nick Daneman, Ross Upshur, Michael Fralick, Lauren Lapointe-Shaw, Terence Tang, Adina Weinerman, Janice L Kwan, Jessica J Liu, Fahad Razak, Amol A Verma
{"title":"Identifying clusters of coexisting conditions and outcomes among adults admitted to hospital with community-acquired pneumonia: a multicentre cohort study.","authors":"Sarah L Malecki, Hae Young Jung, Anne Loffler, Mark A Green, Samir Gupta, Derek MacFadden, Nick Daneman, Ross Upshur, Michael Fralick, Lauren Lapointe-Shaw, Terence Tang, Adina Weinerman, Janice L Kwan, Jessica J Liu, Fahad Razak, Amol A Verma","doi":"10.9778/cmajo.20220193","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Little is known about patterns of coexisting conditions and their influence on clinical care or outcomes in adults admitted to hospital for community-acquired pneumonia (CAP). We sought to evaluate how coexisting conditions cluster in this population to advance understanding of how multimorbidity affects CAP.</p><p><strong>Methods: </strong>We studied 11 085 adults admitted to hospital with CAP at 7 hospitals in Ontario, Canada. Using cluster analysis, we identified patient subgroups based on clustering of comorbidities in the Charlson Comorbidity Index. We derived and replicated cluster analyses in independent cohorts (derivation sample 2010-2015, replication sample 2015-2017), then combined these into a total cohort for final cluster analyses. We described differences in medications, imaging and outcomes.</p><p><strong>Results: </strong>Patients clustered into 7 subgroups. The low comorbidity subgroup (<i>n</i> = 3052, 27.5%) had no comorbidities. The DM-HF-Pulm subgroup had prevalent diabetes, heart failure and chronic lung disease (<i>n</i> = 1710, 15.4%). One disease category defined each remaining subgroup, as follows: pulmonary (<i>n</i> = 1621, 14.6%), diabetes (<i>n</i> = 1281, 11.6%), heart failure (<i>n</i> = 1370, 12.4%), dementia (<i>n</i> = 1038, 9.4%) and cancer (<i>n</i> = 1013, 9.1%). Corticosteroid use ranged from 11.5% to 64.9% in the dementia and pulmonary subgroups, respectively. Piperacillin-tazobactam use ranged from 9.1% to 28.0% in the pulmonary and cancer subgroups, respectively. The use of thoracic computed tomography ranged from 5.7% to 36.3% in the dementia and cancer subgroups, respectively. Adjusting for patient factors, the risk of in-hospital death was greater in the cancer (adjusted odds ratio [OR] 3.12, 95% confidence interval [CI] 2.44-3.99), dementia (adjusted OR 1.57, 95% CI 1.05-2.35), heart failure (adjusted OR 1.66, 95% CI 1.35-2.03) and DM-HF-Pulm subgroups (adjusted OR 1.35, 95% CI 1.12-1.61), and lower in the diabetes subgroup (adjusted OR 0.67, 95% CI 0.50-0.89), compared with the low comorbidity group.</p><p><strong>Interpretation: </strong>Patients admitted to hospital with CAP cluster into clinically recognizable subgroups based on coexisting conditions. Clinical care and outcomes vary among these subgroups with little evidence to guide decision-making, highlighting opportunities for research to personalize care.</p>","PeriodicalId":10432,"journal":{"name":"CMAJ open","volume":"11 5","pages":"E799-E808"},"PeriodicalIF":0.0000,"publicationDate":"2023-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/a5/fd/cmajo.20220193.PMC10482492.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"CMAJ open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.9778/cmajo.20220193","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Little is known about patterns of coexisting conditions and their influence on clinical care or outcomes in adults admitted to hospital for community-acquired pneumonia (CAP). We sought to evaluate how coexisting conditions cluster in this population to advance understanding of how multimorbidity affects CAP.
Methods: We studied 11 085 adults admitted to hospital with CAP at 7 hospitals in Ontario, Canada. Using cluster analysis, we identified patient subgroups based on clustering of comorbidities in the Charlson Comorbidity Index. We derived and replicated cluster analyses in independent cohorts (derivation sample 2010-2015, replication sample 2015-2017), then combined these into a total cohort for final cluster analyses. We described differences in medications, imaging and outcomes.
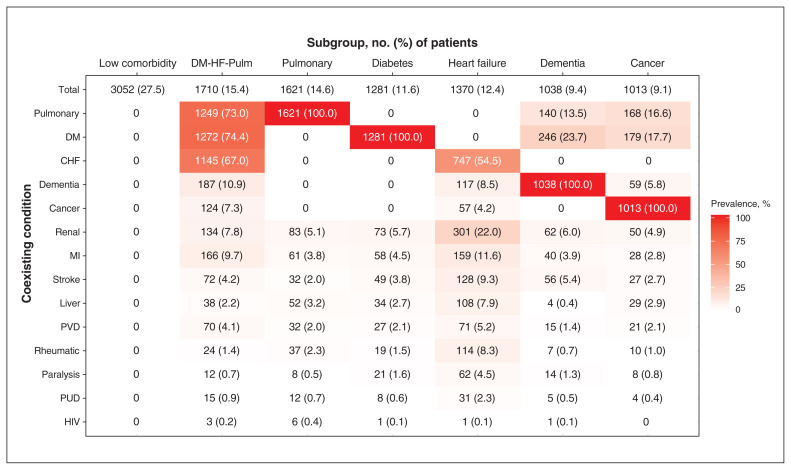
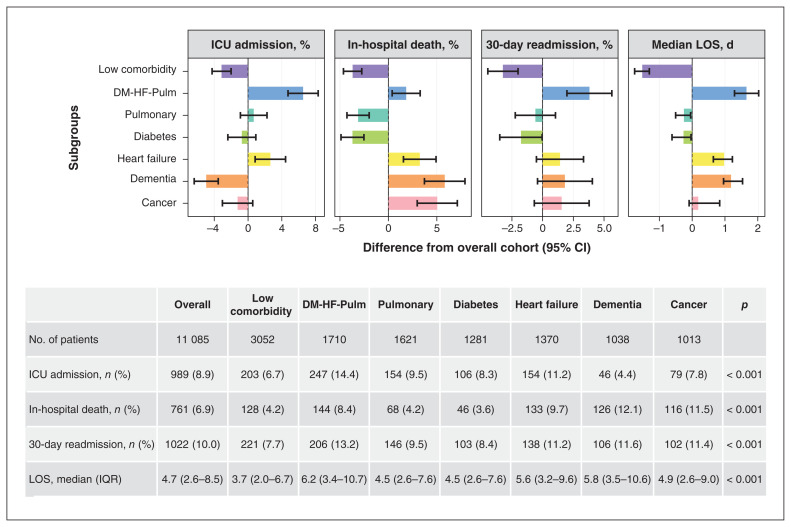
Results: Patients clustered into 7 subgroups. The low comorbidity subgroup (n = 3052, 27.5%) had no comorbidities. The DM-HF-Pulm subgroup had prevalent diabetes, heart failure and chronic lung disease (n = 1710, 15.4%). One disease category defined each remaining subgroup, as follows: pulmonary (n = 1621, 14.6%), diabetes (n = 1281, 11.6%), heart failure (n = 1370, 12.4%), dementia (n = 1038, 9.4%) and cancer (n = 1013, 9.1%). Corticosteroid use ranged from 11.5% to 64.9% in the dementia and pulmonary subgroups, respectively. Piperacillin-tazobactam use ranged from 9.1% to 28.0% in the pulmonary and cancer subgroups, respectively. The use of thoracic computed tomography ranged from 5.7% to 36.3% in the dementia and cancer subgroups, respectively. Adjusting for patient factors, the risk of in-hospital death was greater in the cancer (adjusted odds ratio [OR] 3.12, 95% confidence interval [CI] 2.44-3.99), dementia (adjusted OR 1.57, 95% CI 1.05-2.35), heart failure (adjusted OR 1.66, 95% CI 1.35-2.03) and DM-HF-Pulm subgroups (adjusted OR 1.35, 95% CI 1.12-1.61), and lower in the diabetes subgroup (adjusted OR 0.67, 95% CI 0.50-0.89), compared with the low comorbidity group.
Interpretation: Patients admitted to hospital with CAP cluster into clinically recognizable subgroups based on coexisting conditions. Clinical care and outcomes vary among these subgroups with little evidence to guide decision-making, highlighting opportunities for research to personalize care.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
