Derivation and validation of pragmatic clinical models to predict hospital length of stay after cardiac surgery in Ontario, Canada: a population-based cohort study.
Alexandra Fottinger, Anan Bader Eddeen, Douglas S Lee, Graham Woodward, Louise Y Sun
{"title":"Derivation and validation of pragmatic clinical models to predict hospital length of stay after cardiac surgery in Ontario, Canada: a population-based cohort study.","authors":"Alexandra Fottinger, Anan Bader Eddeen, Douglas S Lee, Graham Woodward, Louise Y Sun","doi":"10.9778/cmajo.20220103","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Cardiac surgery is resource intensive and often requires multidisciplinary involvement to facilitate discharge. To facilitate evidence-based resource planning, we derived and validated clinical models to predict postoperative hospital length of stay (LOS).</p><p><strong>Methods: </strong>We used linked, population-level databases with information on all Ontario residents and included patients aged 18 years or older who underwent coronary artery bypass grafting, valvular or thoracic aorta surgeries between October 2008 and September 2019. The primary outcome was hospital LOS. The models were derived by using patients who had surgery before Sept. 30, 2016, and validated after that date. To address the rightward skew in LOS data and to identify top-tier resource users, we used logistic regression to derive a model to predict the likelihood of LOS being more than the 98th percentile (> 30 d), and γ regression in the remainder to predict continuous LOS in days. We used backward stepwise variable selection for both models.</p><p><strong>Results: </strong>Among 105 193 patients, 2422 (2.3%) had an LOS of more than 30 days. Factors predicting prolonged LOS included age, female sex, procedure type and urgency, comorbidities including frailty, high-risk acute coronary syndrome, heart failure, reduced left ventricular ejection fraction and psychiatric and pulmonary circulatory disease. The C statistic was 0.92 for the prolonged LOS model and the mean absolute error was 2.4 days for the continuous LOS model.</p><p><strong>Interpretation: </strong>We derived and validated clinical models to identify top-tier resource users and predict continuous LOS with excellent accuracy. Our models could be used to benchmark clinical performance based on expected LOS, rationally allocate resources and support patient-centred operative decision-making.</p>","PeriodicalId":10432,"journal":{"name":"CMAJ open","volume":"11 1","pages":"E180-E190"},"PeriodicalIF":0.0000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/28/e3/cmajo.20220103.PMC9981165.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"CMAJ open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.9778/cmajo.20220103","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Cardiac surgery is resource intensive and often requires multidisciplinary involvement to facilitate discharge. To facilitate evidence-based resource planning, we derived and validated clinical models to predict postoperative hospital length of stay (LOS).
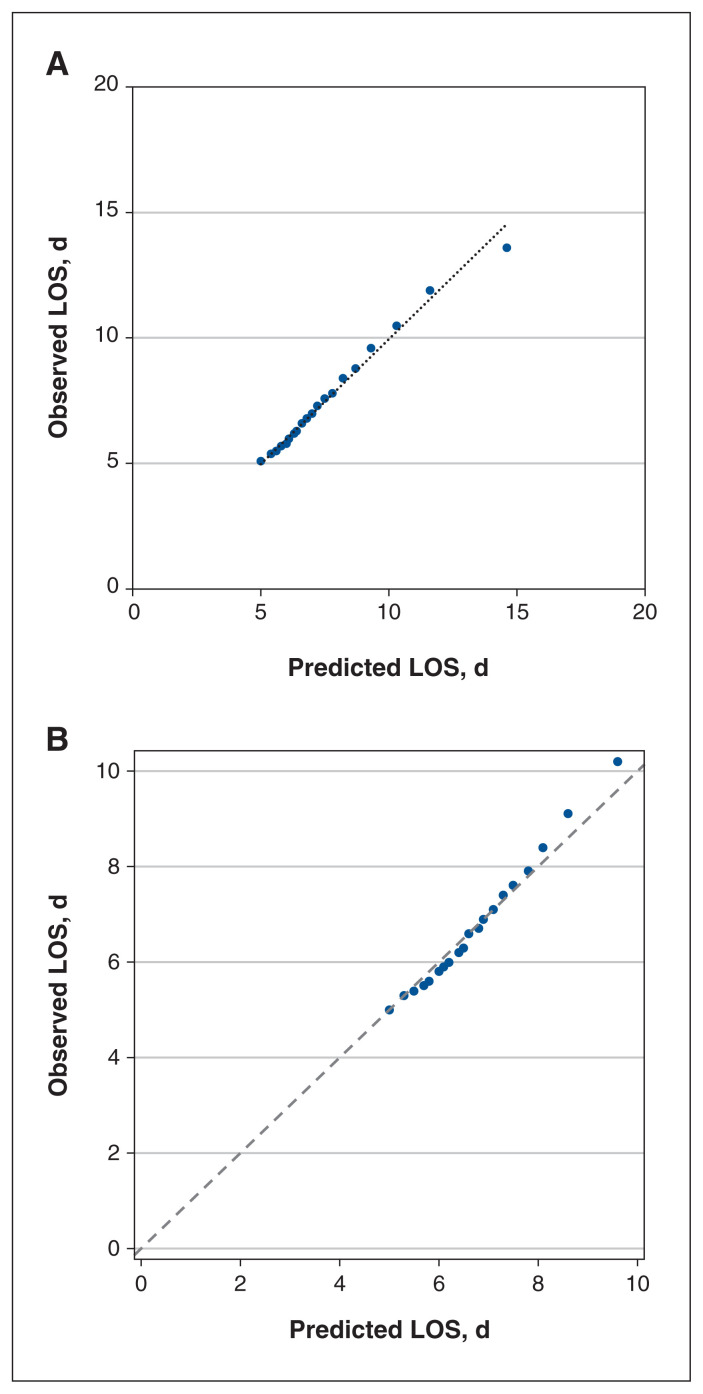
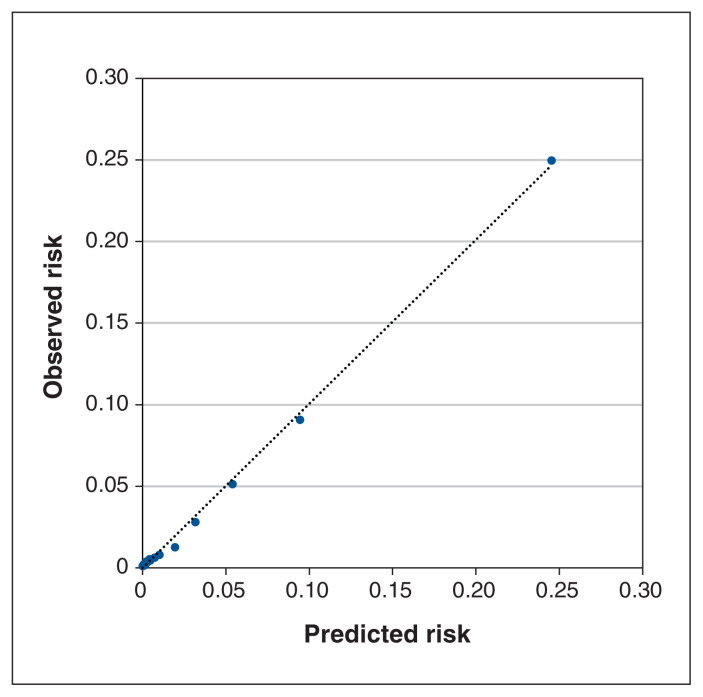
Methods: We used linked, population-level databases with information on all Ontario residents and included patients aged 18 years or older who underwent coronary artery bypass grafting, valvular or thoracic aorta surgeries between October 2008 and September 2019. The primary outcome was hospital LOS. The models were derived by using patients who had surgery before Sept. 30, 2016, and validated after that date. To address the rightward skew in LOS data and to identify top-tier resource users, we used logistic regression to derive a model to predict the likelihood of LOS being more than the 98th percentile (> 30 d), and γ regression in the remainder to predict continuous LOS in days. We used backward stepwise variable selection for both models.
Results: Among 105 193 patients, 2422 (2.3%) had an LOS of more than 30 days. Factors predicting prolonged LOS included age, female sex, procedure type and urgency, comorbidities including frailty, high-risk acute coronary syndrome, heart failure, reduced left ventricular ejection fraction and psychiatric and pulmonary circulatory disease. The C statistic was 0.92 for the prolonged LOS model and the mean absolute error was 2.4 days for the continuous LOS model.
Interpretation: We derived and validated clinical models to identify top-tier resource users and predict continuous LOS with excellent accuracy. Our models could be used to benchmark clinical performance based on expected LOS, rationally allocate resources and support patient-centred operative decision-making.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
