Kevin Verhoeff, Alexandria N Webb, Daniel Krys, Danielle Anderson, David L Bigam, Christopher I Fung
{"title":"Multicentre Analysis of Cost, Uptake and Safety of Canadian Multidisciplinary Pancreatic Cyst Guidelines.","authors":"Kevin Verhoeff, Alexandria N Webb, Daniel Krys, Danielle Anderson, David L Bigam, Christopher I Fung","doi":"10.1093/jcag/gwad001","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Pancreatic cystic lesions (PCLs) are common, with several guidelines providing surveillance recommendations. The Canadian Association of Radiologists published surveillance guidelines (CARGs) intended to provide simplified, cost-effective and safe recommendations. This study aimed to evaluate cost savings of CARGs compared to other North American guidelines including American Gastroenterology Association guidelines (AGAG) and American College of Radiology guidelines (ACRG), and to evaluate CARG safety and uptake.</p><p><strong>Methods: </strong>This is a multicentre retrospective study evaluating adults with PCL from a single health zone. MRIs completed from September 2018-2019, one year after local CARG guideline implementation, were reviewed to identify PCLs. All imaging following 3-4 years of CARG implementation was reviewed to evaluate true costs, missed malignancy and guideline uptake. Modelling, including MRI and consultation, predicted and compared costs associated with surveillance based on CARGs, AGAGs and ACRGs.</p><p><strong>Results: </strong>6698 abdominal MRIs were reviewed with 1001 (14.9%) identifying PCL. Application of CARGs over 3.1 years demonstrated a >70% cost reduction compared to other guidelines. Similarly, the modelled cost of surveillance for 10-years for each guideline was $516,183, $1,908,425 and $1,924,607 for CARGs, AGAGs and ACRGs respectively. Of patients suggested to not require further surveillance per CARGs, approximately 1% develop malignancy with fewer being candidates for surgical resection. Overall, 44.8% of initial PCL reports provided CARG recommendations while 54.3% of PCLs were followed as per CARGs.</p><p><strong>Conclusions: </strong>CARGs are safe and offer substantial cost and opportunity savings for PCL surveillance. These findings support Canada-wide implementation with close monitoring of consultation requirements and missed diagnoses.</p>","PeriodicalId":17263,"journal":{"name":"Journal of the Canadian Association of Gastroenterology","volume":"6 2","pages":"86-93"},"PeriodicalIF":2.7000,"publicationDate":"2023-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10071295/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of the Canadian Association of Gastroenterology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/jcag/gwad001","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
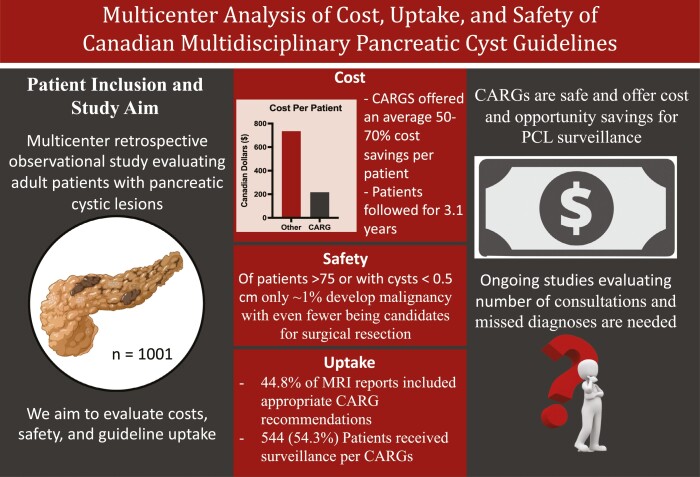
Background: Pancreatic cystic lesions (PCLs) are common, with several guidelines providing surveillance recommendations. The Canadian Association of Radiologists published surveillance guidelines (CARGs) intended to provide simplified, cost-effective and safe recommendations. This study aimed to evaluate cost savings of CARGs compared to other North American guidelines including American Gastroenterology Association guidelines (AGAG) and American College of Radiology guidelines (ACRG), and to evaluate CARG safety and uptake.
Methods: This is a multicentre retrospective study evaluating adults with PCL from a single health zone. MRIs completed from September 2018-2019, one year after local CARG guideline implementation, were reviewed to identify PCLs. All imaging following 3-4 years of CARG implementation was reviewed to evaluate true costs, missed malignancy and guideline uptake. Modelling, including MRI and consultation, predicted and compared costs associated with surveillance based on CARGs, AGAGs and ACRGs.
Results: 6698 abdominal MRIs were reviewed with 1001 (14.9%) identifying PCL. Application of CARGs over 3.1 years demonstrated a >70% cost reduction compared to other guidelines. Similarly, the modelled cost of surveillance for 10-years for each guideline was $516,183, $1,908,425 and $1,924,607 for CARGs, AGAGs and ACRGs respectively. Of patients suggested to not require further surveillance per CARGs, approximately 1% develop malignancy with fewer being candidates for surgical resection. Overall, 44.8% of initial PCL reports provided CARG recommendations while 54.3% of PCLs were followed as per CARGs.
Conclusions: CARGs are safe and offer substantial cost and opportunity savings for PCL surveillance. These findings support Canada-wide implementation with close monitoring of consultation requirements and missed diagnoses.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
