Medical therapy versus percutaneous coronary intervention or coronary artery bypass graft in stable coronary artery disease; a systematic review and meta-analysis of randomized clinical trials.
{"title":"Medical therapy versus percutaneous coronary intervention or coronary artery bypass graft in stable coronary artery disease; a systematic review and meta-analysis of randomized clinical trials.","authors":"Majid Davari, Mende Mensa Sorato, Behzad Fatemi, Soheila Rezaei, Hamid Sanei","doi":"10.48305/arya.2022.24252","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Ischemic heart disease (IHD) is the first cause of mortality in the world. Stable coronary artery disease (CAD) is the most common IHD. Medical therapy (MT), percutaneous coronary intervention (PCI), and coronary artery bypass grafting (CABG) are three strategies for the management of this disease. The main aim of this study was the comparison of MT with PCI or CABG in terms of cardiovascular (CV) mortality, myocardial infarction (MI), unplanned revascularization (UR), stroke, and freedom from angina in managing stable CAD.</p><p><strong>Methods: </strong>The Cochrane Central Register of Controlled Trials, Embase, PubMed, and Scopus were searched. Two reviewers independently appraised the titles and abstracted data of the identified studies. After the Full-text reviewing phase, eligible studies were analyzed through the random-effect meta-analysis method. Finally, a sensitivity analysis was conducted for the robustness of findings.</p><p><strong>Results: </strong>Nine randomized controlled trials (RCTs) were included. The pooled RR of CV mortality associated with MT compared with PCI and CABG was 1.22 and 1.385, respectively. Overall, The RR of MT associated with MI, UR, stroke, and freedom from angina compared with PCI was 1.001, 1.151, 0.799, and 0.801, respectively.</p><p><strong>Conclusion: </strong>Our results revealed no statistically significant difference between MT and PCI in terms of studied primary outcomes. The findings also highlighted that there is no statistically significant difference between MT and CABG in terms of CV mortality.</p>","PeriodicalId":46477,"journal":{"name":"ARYA Atherosclerosis","volume":"18 3","pages":"1-12"},"PeriodicalIF":0.6000,"publicationDate":"2022-05-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/26/0d/ARYA-18-8-2288.PMC9931946.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"ARYA Atherosclerosis","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.48305/arya.2022.24252","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Ischemic heart disease (IHD) is the first cause of mortality in the world. Stable coronary artery disease (CAD) is the most common IHD. Medical therapy (MT), percutaneous coronary intervention (PCI), and coronary artery bypass grafting (CABG) are three strategies for the management of this disease. The main aim of this study was the comparison of MT with PCI or CABG in terms of cardiovascular (CV) mortality, myocardial infarction (MI), unplanned revascularization (UR), stroke, and freedom from angina in managing stable CAD.
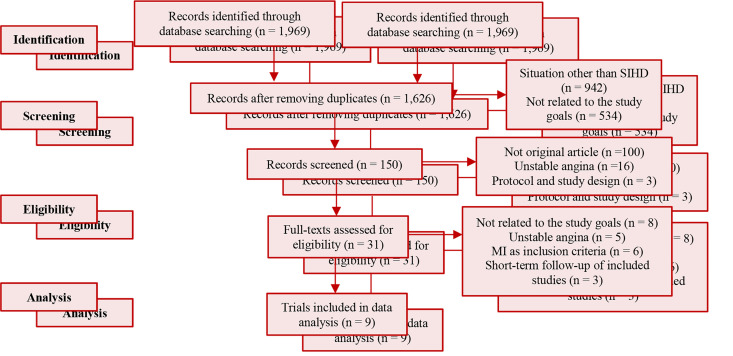
Methods: The Cochrane Central Register of Controlled Trials, Embase, PubMed, and Scopus were searched. Two reviewers independently appraised the titles and abstracted data of the identified studies. After the Full-text reviewing phase, eligible studies were analyzed through the random-effect meta-analysis method. Finally, a sensitivity analysis was conducted for the robustness of findings.
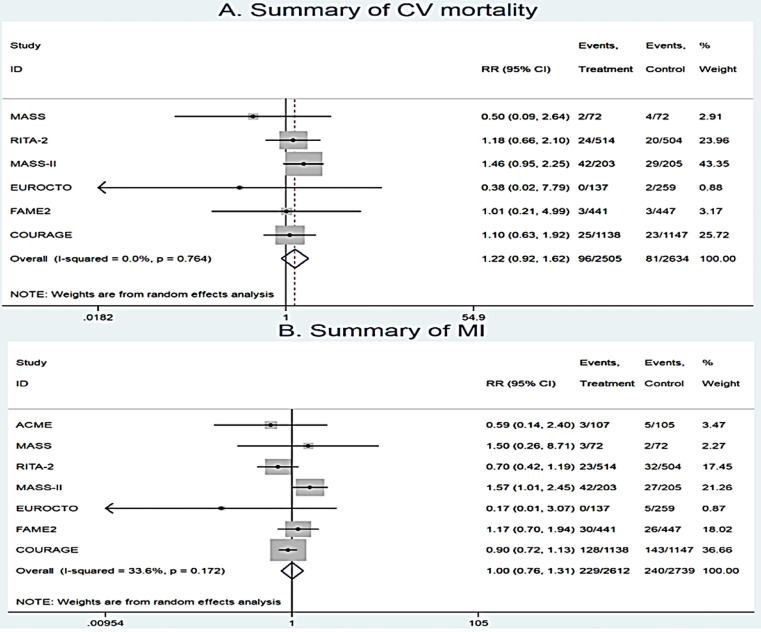
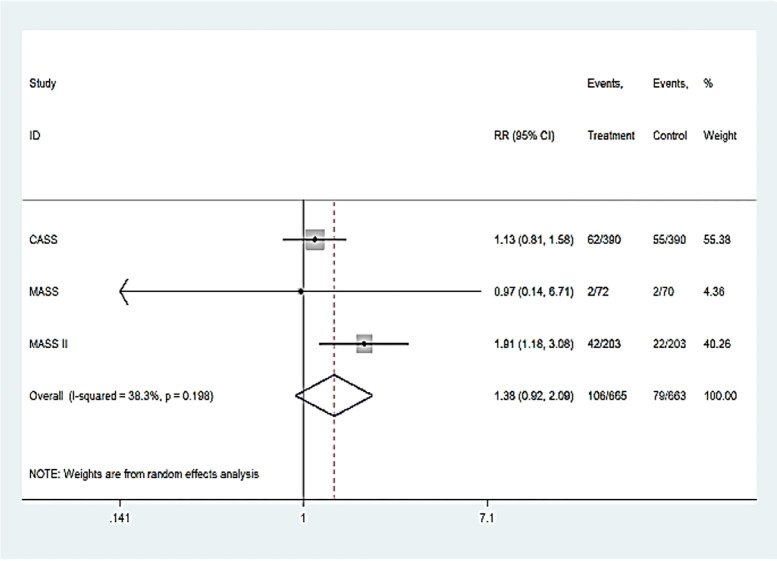
Results: Nine randomized controlled trials (RCTs) were included. The pooled RR of CV mortality associated with MT compared with PCI and CABG was 1.22 and 1.385, respectively. Overall, The RR of MT associated with MI, UR, stroke, and freedom from angina compared with PCI was 1.001, 1.151, 0.799, and 0.801, respectively.
Conclusion: Our results revealed no statistically significant difference between MT and PCI in terms of studied primary outcomes. The findings also highlighted that there is no statistically significant difference between MT and CABG in terms of CV mortality.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
