Niels Vanvelk, Esther M M Van Lieshout, Jolien Onsea, Jonathan Sliepen, Geertje Govaert, Frank F A IJpma, Melissa Depypere, Jamie Ferguson, Martin McNally, William T Obremskey, Charalampos Zalavras, Michael H J Verhofstad, Willem-Jan Metsemakers
{"title":"Diagnosis of fracture-related infection in patients without clinical confirmatory criteria: an international retrospective cohort study.","authors":"Niels Vanvelk, Esther M M Van Lieshout, Jolien Onsea, Jonathan Sliepen, Geertje Govaert, Frank F A IJpma, Melissa Depypere, Jamie Ferguson, Martin McNally, William T Obremskey, Charalampos Zalavras, Michael H J Verhofstad, Willem-Jan Metsemakers","doi":"10.5194/jbji-8-133-2023","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background</b>: fracture-related infection (FRI) remains a serious complication in orthopedic trauma. To standardize daily clinical practice, a consensus definition was established, based on confirmatory and suggestive criteria. In the presence of clinical confirmatory criteria, the diagnosis of an FRI is evident, and treatment can be started. However, if these criteria are absent, the decision to surgically collect deep tissue cultures can only be based on suggestive criteria. The primary study aim was to characterize the subpopulation of FRI patients presenting without clinical confirmatory criteria (fistula, sinus, wound breakdown, purulent wound drainage or presence of pus during surgery). The secondary aims were to describe the prevalence of the diagnostic criteria for FRI and present the microbiological characteristics, both for the entire FRI population. <b>Methods</b>: a multicenter, retrospective cohort study was performed, reporting the demographic, clinical and microbiological characteristics of 609 patients (with 613 fractures) who were treated for FRI based on the recommendations of a multidisciplinary team. Patients were divided in three groups, including the total population and two subgroups of patients presenting with or without clinical confirmatory criteria. <b>Results</b>: clinical and microbiological confirmatory criteria were present in 77 % and 87 % of the included fractures, respectively. Of patients, 23 % presented without clinical confirmatory criteria, and they mostly displayed one (31 %) or two (23 %) suggestive clinical criteria (redness, swelling, warmth, pain, fever, new-onset joint effusion, persisting/increasing/new-onset wound drainage). The prevalence of any suggestive clinical, radiological or laboratory criteria in this subgroup was 85 %, 55 % and 97 %, respectively. Most infections were monomicrobial (64 %) and caused by <i>Staphylococcus aureus</i>. <b>Conclusion</b>: clinical confirmatory criteria were absent in 23 % of the FRIs. In these cases, the decision to operatively collect deep tissue cultures was based on clinical, radiological and laboratory suggestive criteria. The combined use of these criteria should guide physicians in the management pathway of FRI. Further research is needed to provide guidelines on the decision to proceed with surgery when only these suggestive criteria are present.</p>","PeriodicalId":15271,"journal":{"name":"Journal of Bone and Joint Infection","volume":"8 2","pages":"133-142"},"PeriodicalIF":2.8000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10134751/pdf/","citationCount":"3","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Bone and Joint Infection","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5194/jbji-8-133-2023","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"INFECTIOUS DISEASES","Score":null,"Total":0}
引用次数: 3
Abstract
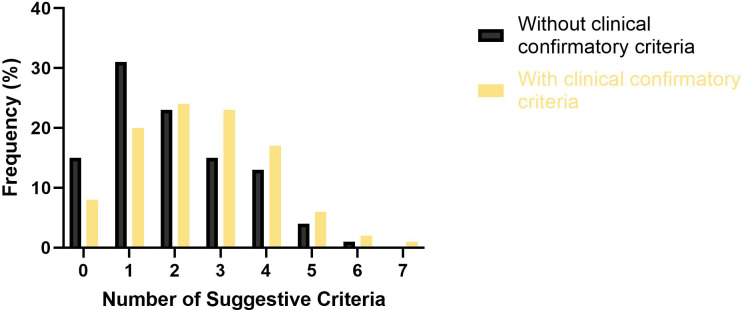
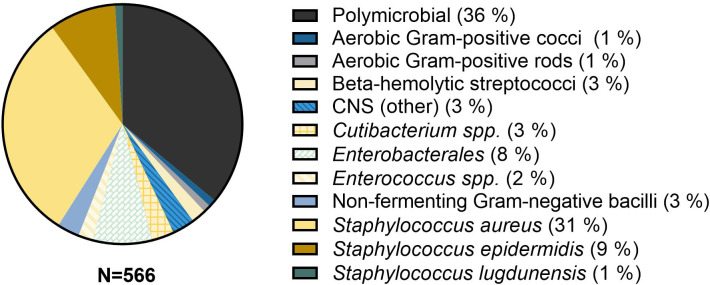
Background: fracture-related infection (FRI) remains a serious complication in orthopedic trauma. To standardize daily clinical practice, a consensus definition was established, based on confirmatory and suggestive criteria. In the presence of clinical confirmatory criteria, the diagnosis of an FRI is evident, and treatment can be started. However, if these criteria are absent, the decision to surgically collect deep tissue cultures can only be based on suggestive criteria. The primary study aim was to characterize the subpopulation of FRI patients presenting without clinical confirmatory criteria (fistula, sinus, wound breakdown, purulent wound drainage or presence of pus during surgery). The secondary aims were to describe the prevalence of the diagnostic criteria for FRI and present the microbiological characteristics, both for the entire FRI population. Methods: a multicenter, retrospective cohort study was performed, reporting the demographic, clinical and microbiological characteristics of 609 patients (with 613 fractures) who were treated for FRI based on the recommendations of a multidisciplinary team. Patients were divided in three groups, including the total population and two subgroups of patients presenting with or without clinical confirmatory criteria. Results: clinical and microbiological confirmatory criteria were present in 77 % and 87 % of the included fractures, respectively. Of patients, 23 % presented without clinical confirmatory criteria, and they mostly displayed one (31 %) or two (23 %) suggestive clinical criteria (redness, swelling, warmth, pain, fever, new-onset joint effusion, persisting/increasing/new-onset wound drainage). The prevalence of any suggestive clinical, radiological or laboratory criteria in this subgroup was 85 %, 55 % and 97 %, respectively. Most infections were monomicrobial (64 %) and caused by Staphylococcus aureus. Conclusion: clinical confirmatory criteria were absent in 23 % of the FRIs. In these cases, the decision to operatively collect deep tissue cultures was based on clinical, radiological and laboratory suggestive criteria. The combined use of these criteria should guide physicians in the management pathway of FRI. Further research is needed to provide guidelines on the decision to proceed with surgery when only these suggestive criteria are present.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
