{"title":"Resection of Cervical Dumbbell-Shaped Schwannoma Using Posterior Unilateral Approach: Impact on Postoperative Cervical Function and Clinical Outcomes.","authors":"Toshiki Okubo, Narihito Nagoshi, Osahiko Tsuji, Satoshi Suzuki, Yohei Takahashi, Mitsuru Yagi, Morio Matsumoto, Masaya Nakamura, Kota Watanabe","doi":"10.1177/21925682231178205","DOIUrl":null,"url":null,"abstract":"<p><strong>Study design: </strong>A retrospective comparative study.</p><p><strong>Objectives: </strong>This study aimed to evaluate the radiographical changes in cervical sagittal alignment (CSA) and clinical outcomes after tumor resection using a posterior unilateral approach without spinal fixation for patients with cervical dumbbell-shaped schwannoma (DS).</p><p><strong>Methods: </strong>Seventy-three patients with DS who were followed up for at least 2 years were included. The Eden classification was used to designate the types of DS. The CSA and range of motion (ROM) were analyzed using radiographs. The clinical outcomes were assessed using the Japanese Orthopaedic Association (JOA) score and JOA cervical myelopathy questionnaire.</p><p><strong>Results: </strong>The CSA in the neutral, flexion, and extension position and cervical ROM were not significantly reduced in the follow-up period. The JOA scores showed significant improvement after surgery. The postoperative radiographic parameters and clinical outcomes of Eden type II or III DS, which needed facetectomy for the resection, did not show any statistically significant difference compared with those of Eden type I tumor, which was resected without facetectomy. Fifty-two cases (71.2%) achieved gross total resection, whereas 21 cases (28.8%) remained in partial resection (PR). One case underwent reoperation due to the regrowth of the remnant tumor whose margin was at the entrance of the intervertebral foramen.</p><p><strong>Conclusions: </strong>Tumor resection using the posterior unilateral approach preserved CSA and resulted in favorable clinical outcomes in patients with DS. When the resection ends in PR, the proximal margin of the remnant tumor should be located distally away from the entrance of the foramen to prevent regrowth.</p>","PeriodicalId":12680,"journal":{"name":"Global Spine Journal","volume":" ","pages":"2317-2326"},"PeriodicalIF":3.0000,"publicationDate":"2024-11-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11529086/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Global Spine Journal","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/21925682231178205","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/5/21 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Study design: A retrospective comparative study.
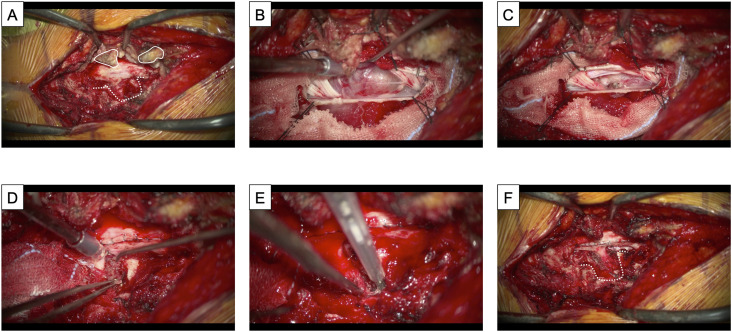
Objectives: This study aimed to evaluate the radiographical changes in cervical sagittal alignment (CSA) and clinical outcomes after tumor resection using a posterior unilateral approach without spinal fixation for patients with cervical dumbbell-shaped schwannoma (DS).
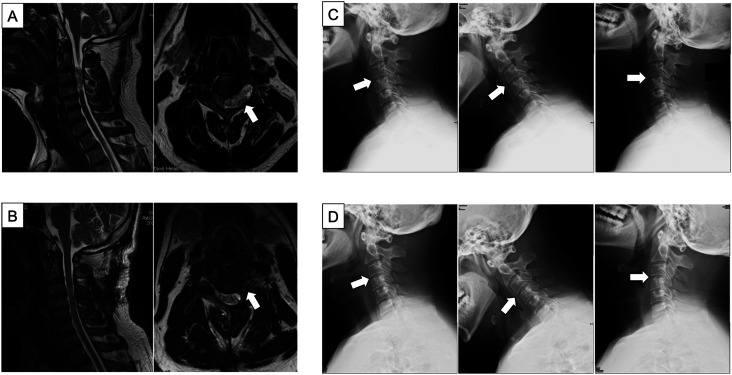
Methods: Seventy-three patients with DS who were followed up for at least 2 years were included. The Eden classification was used to designate the types of DS. The CSA and range of motion (ROM) were analyzed using radiographs. The clinical outcomes were assessed using the Japanese Orthopaedic Association (JOA) score and JOA cervical myelopathy questionnaire.
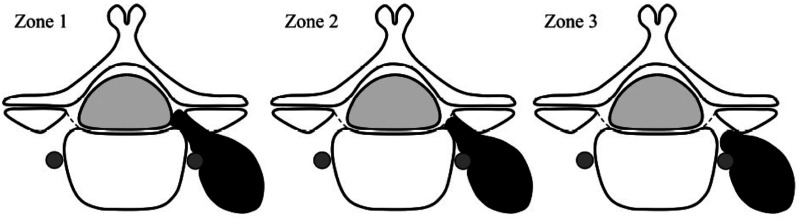
Results: The CSA in the neutral, flexion, and extension position and cervical ROM were not significantly reduced in the follow-up period. The JOA scores showed significant improvement after surgery. The postoperative radiographic parameters and clinical outcomes of Eden type II or III DS, which needed facetectomy for the resection, did not show any statistically significant difference compared with those of Eden type I tumor, which was resected without facetectomy. Fifty-two cases (71.2%) achieved gross total resection, whereas 21 cases (28.8%) remained in partial resection (PR). One case underwent reoperation due to the regrowth of the remnant tumor whose margin was at the entrance of the intervertebral foramen.
Conclusions: Tumor resection using the posterior unilateral approach preserved CSA and resulted in favorable clinical outcomes in patients with DS. When the resection ends in PR, the proximal margin of the remnant tumor should be located distally away from the entrance of the foramen to prevent regrowth.
期刊介绍:
Global Spine Journal (GSJ) is the official scientific publication of AOSpine. A peer-reviewed, open access journal, devoted to the study and treatment of spinal disorders, including diagnosis, operative and non-operative treatment options, surgical techniques, and emerging research and clinical developments.GSJ is indexed in PubMedCentral, SCOPUS, and Emerging Sources Citation Index (ESCI).



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
