Uwe Walter, Erik Volmer, Matthias Wittstock, Alexander Storch, Marc-André Weber, Annette Großmann
{"title":"[Cerebral venous sinus thrombosis after COVID-19 vaccination : Neurological and radiological management].","authors":"Uwe Walter, Erik Volmer, Matthias Wittstock, Alexander Storch, Marc-André Weber, Annette Großmann","doi":"10.1007/s00117-021-00887-3","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Vaccine-induced cerebral venous and sinus thrombosis (VI-CVST) is a rare complication in recipients of the adenovirus-vectored coronavirus disease 2019 (COVID-19) vaccine ChAdOx1 nCov-19 (Vaxzevria®; AstraZeneca).</p><p><strong>Objectives: </strong>Development of a diagnostic and therapeutic standard.</p><p><strong>Materials and methods: </strong>Analysis of clinical and basic research findings, expert opinions, and experience with our own cases.</p><p><strong>Results: </strong>VI-CVST usually manifests on day 4-24 after vaccination, mostly in individuals aged < 60 years, and women. In the majority there is an immune pathogenesis caused by antibodies against platelet factor 4/polyanion complexes, leading to thrombotic thrombocytopenia which can result in severe, sometimes fatal, course. The cardinal symptom is headache worsening within days which, however, also can be of variable intensity. Other possible symptoms are seizures, visual disturbance, focal neurological deficits and signs of increased intracranial pressure. If VI-CVST is suspected, the determination of plasma D‑dimer level, platelet count, and screening for heparin-induced thrombocytopenia (HIT-2) are essential for treatment decision-making. Magnetic resonance imaging (MRI) with venous MR-angiography is the neuroimaging modality of choice to confirm or exclude VI-CVST. On T2* susceptibility-weighted MRI, the clot in the sinuses or veins produces marked susceptibility artifacts (\"blooming\"), which also enables the detection of isolated cortical venous thromboses. MRI/MR-angiography or computed tomography (CT)/CT-angiography usually allow-in combination with clinical and laboratory findings-reliable diagnosis of VI-CVST.</p><p><strong>Conclusions: </strong>The clinical suspicion of VI-CVST calls for urgent laboratory and neuroimaging workup. In the presence of thrombocytopenia and/or pathogenic antibodies, specific medications for anticoagulation and immunomodulation are recommended.</p>","PeriodicalId":54513,"journal":{"name":"Radiologe","volume":"61 10","pages":"923-932"},"PeriodicalIF":0.0000,"publicationDate":"2021-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8320717/pdf/","citationCount":"5","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Radiologe","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s00117-021-00887-3","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 5
Abstract
Background: Vaccine-induced cerebral venous and sinus thrombosis (VI-CVST) is a rare complication in recipients of the adenovirus-vectored coronavirus disease 2019 (COVID-19) vaccine ChAdOx1 nCov-19 (Vaxzevria®; AstraZeneca).
Objectives: Development of a diagnostic and therapeutic standard.
Materials and methods: Analysis of clinical and basic research findings, expert opinions, and experience with our own cases.
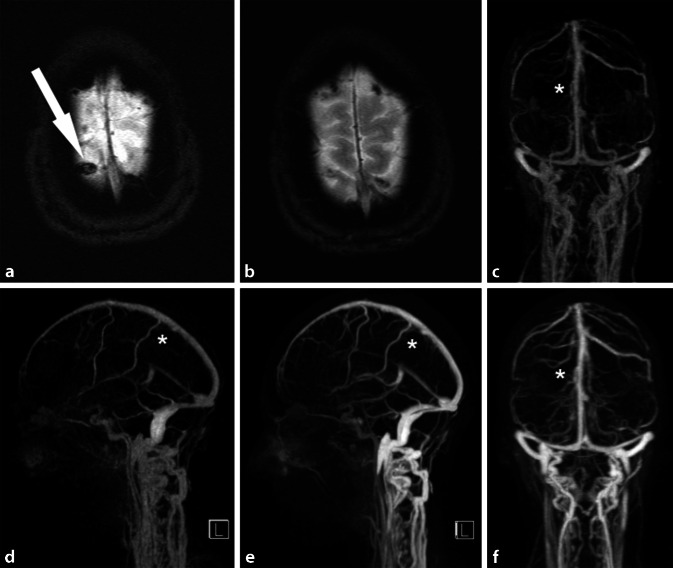
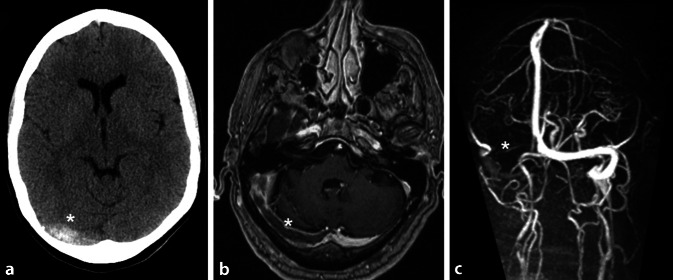
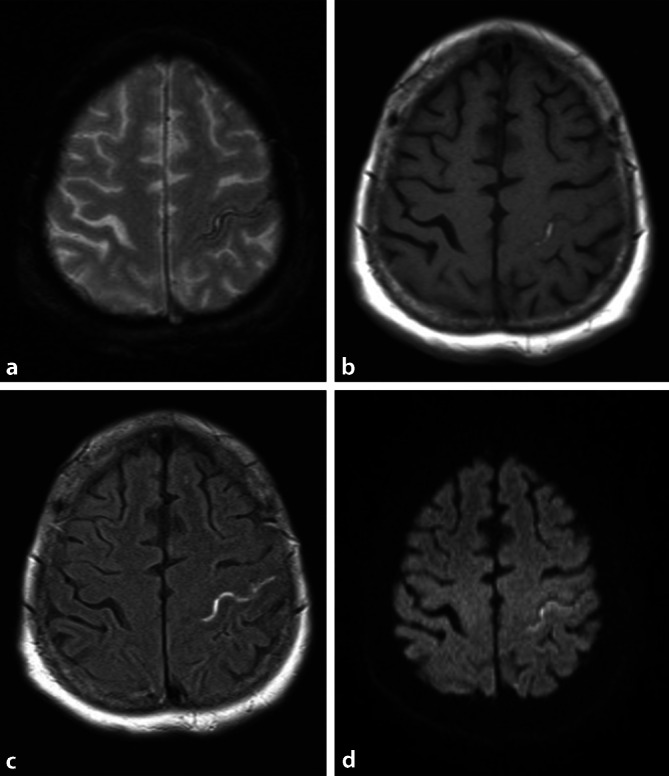
Results: VI-CVST usually manifests on day 4-24 after vaccination, mostly in individuals aged < 60 years, and women. In the majority there is an immune pathogenesis caused by antibodies against platelet factor 4/polyanion complexes, leading to thrombotic thrombocytopenia which can result in severe, sometimes fatal, course. The cardinal symptom is headache worsening within days which, however, also can be of variable intensity. Other possible symptoms are seizures, visual disturbance, focal neurological deficits and signs of increased intracranial pressure. If VI-CVST is suspected, the determination of plasma D‑dimer level, platelet count, and screening for heparin-induced thrombocytopenia (HIT-2) are essential for treatment decision-making. Magnetic resonance imaging (MRI) with venous MR-angiography is the neuroimaging modality of choice to confirm or exclude VI-CVST. On T2* susceptibility-weighted MRI, the clot in the sinuses or veins produces marked susceptibility artifacts ("blooming"), which also enables the detection of isolated cortical venous thromboses. MRI/MR-angiography or computed tomography (CT)/CT-angiography usually allow-in combination with clinical and laboratory findings-reliable diagnosis of VI-CVST.
Conclusions: The clinical suspicion of VI-CVST calls for urgent laboratory and neuroimaging workup. In the presence of thrombocytopenia and/or pathogenic antibodies, specific medications for anticoagulation and immunomodulation are recommended.
期刊介绍:
Der Radiologe is an internationally recognized journal dealing with all aspects of radiology and serving the continuing medical education of radiologists in clinical and practical environments. The focus is on x-ray diagnostics, angiography computer tomography, interventional radiology, magnet resonance tomography, digital picture processing, radio oncology and nuclear medicine.
Comprehensive reviews on a specific topical issue focus on providing evidenced based information on diagnostics and therapy.
Freely submitted original papers allow the presentation of important clinical studies and serve the scientific exchange.
Review articles under the rubric ''Continuing Medical Education'' present verified results of scientific research and their integration into daily practice.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
