The effect of a specialist paramedic primary care rotation on appropriate non-conveyance decisions (SPRAINED) study: a controlled interrupted time series analysis.
{"title":"The effect of a specialist paramedic primary care rotation on appropriate non-conveyance decisions (SPRAINED) study: a controlled interrupted time series analysis.","authors":"Richard Pilbery, Tracey Young, Andrew Hodge","doi":"10.29045/14784726.2022.06.7.1.9","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>NHS ambulance service non-conveyance rates in the United Kingdom are around 30%, despite an increase in non-emergency cases and a national policy of integrating urgent and emergency care to provide patients with the 'right care, in the right place, at the right time'. Emergency department overcrowding is a significant issue for patients, resulting in poorer quality of care, increased healthcare costs and potentially, increased mortality. It also contributes to increased ambulance turnaround times. Yorkshire Ambulance Service NHS Trust (YAS) introduced a specialist paramedic (SP) to improve the management of lower acuity cases, but non-conveyance rates in this group have not been as high as expected.In 2018, Health Education England funded a pilot scheme to rotate paramedics into a range of healthcare settings and in YAS, 10 SPs undertook a 10-week placement in a GP practice. This study aimed to evaluate whether a primary care placement appropriately increased the level and trend of non-conveyance decisions made by SPs following a 10-week GP placement, in a cost-effective manner.</p><p><strong>Methods: </strong>We conducted a controlled interrupted time series analysis using data from incidents between 1 June 2017 and 31 December 2019, to study appropriate non-conveyance rates before and after a GP placement. A costing analysis, examining the average cost per appropriate non-conveyance achieved for patients receiving care from intervention group SPs pre- and post-placement, was also conducted.</p><p><strong>Results: </strong>A total of 7349 incidents attended by intervention group SPs were eligible for inclusion. Following removal of cases with missing data, 5537 (75.3%) cases remained. Post-placement, the intervention group demonstrated an increase in appropriate non-conveyance rate of 35.0% (95% CI 23.8%-46.2%), and a reduction in the trend of appropriate non-conveyance of -1.2% (95% CI -2.8%-0.5%), relative to the control group.Post-placement, the cost per appropriate non-conveyance for intervention group SPs was a mean of £509.41 (95% bootstrapped CI £454.92-£564.26) versus £1257.81 (95% bootstrapped CI £1233.42-£1283.95) for the same group in the pre-placement phase.</p><p><strong>Conclusion: </strong>In this single UK NHS ambulance service study, we found a clinically important and statistically significant increase in appropriate non-conveyance rates by SPs who had completed a 10-week GP placement. This improvement persisted for the 12-month period following the placement and demonstrated cost savings compared to usual care.</p>","PeriodicalId":72470,"journal":{"name":"British paramedic journal","volume":"7 1","pages":"9-18"},"PeriodicalIF":0.0000,"publicationDate":"2022-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9662143/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"British paramedic journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.29045/14784726.2022.06.7.1.9","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: NHS ambulance service non-conveyance rates in the United Kingdom are around 30%, despite an increase in non-emergency cases and a national policy of integrating urgent and emergency care to provide patients with the 'right care, in the right place, at the right time'. Emergency department overcrowding is a significant issue for patients, resulting in poorer quality of care, increased healthcare costs and potentially, increased mortality. It also contributes to increased ambulance turnaround times. Yorkshire Ambulance Service NHS Trust (YAS) introduced a specialist paramedic (SP) to improve the management of lower acuity cases, but non-conveyance rates in this group have not been as high as expected.In 2018, Health Education England funded a pilot scheme to rotate paramedics into a range of healthcare settings and in YAS, 10 SPs undertook a 10-week placement in a GP practice. This study aimed to evaluate whether a primary care placement appropriately increased the level and trend of non-conveyance decisions made by SPs following a 10-week GP placement, in a cost-effective manner.
Methods: We conducted a controlled interrupted time series analysis using data from incidents between 1 June 2017 and 31 December 2019, to study appropriate non-conveyance rates before and after a GP placement. A costing analysis, examining the average cost per appropriate non-conveyance achieved for patients receiving care from intervention group SPs pre- and post-placement, was also conducted.
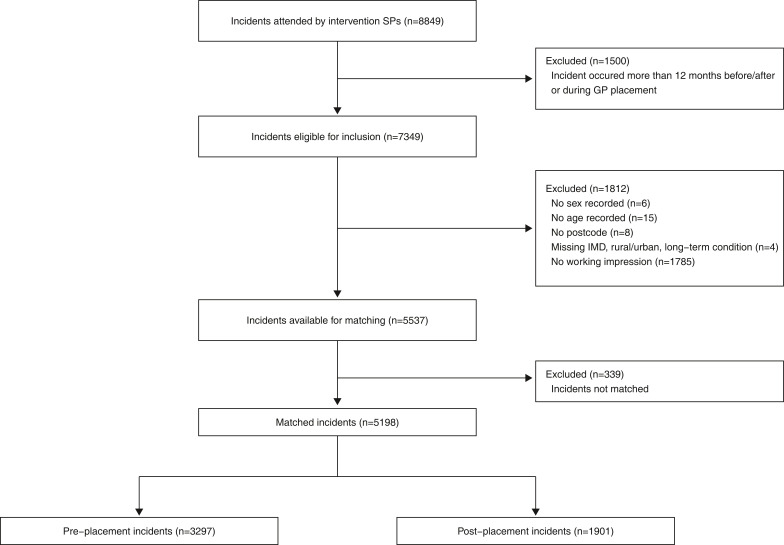
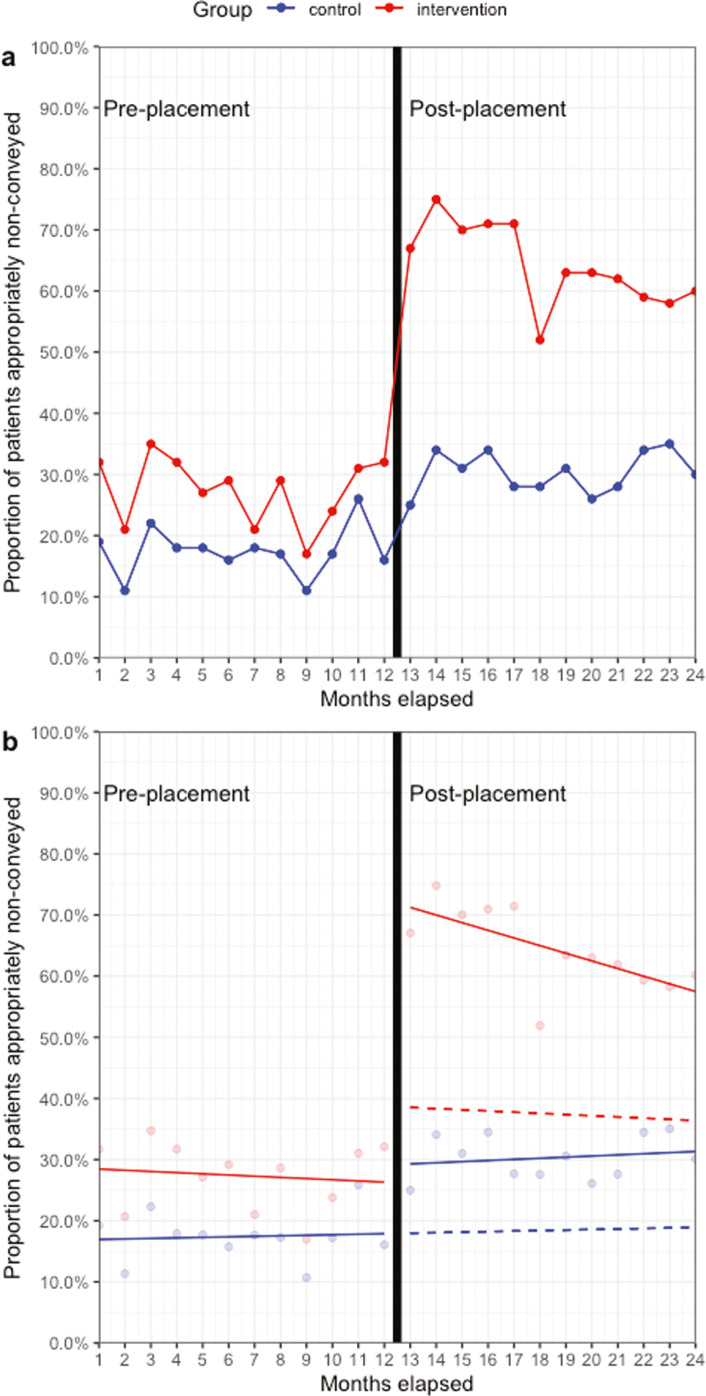
Results: A total of 7349 incidents attended by intervention group SPs were eligible for inclusion. Following removal of cases with missing data, 5537 (75.3%) cases remained. Post-placement, the intervention group demonstrated an increase in appropriate non-conveyance rate of 35.0% (95% CI 23.8%-46.2%), and a reduction in the trend of appropriate non-conveyance of -1.2% (95% CI -2.8%-0.5%), relative to the control group.Post-placement, the cost per appropriate non-conveyance for intervention group SPs was a mean of £509.41 (95% bootstrapped CI £454.92-£564.26) versus £1257.81 (95% bootstrapped CI £1233.42-£1283.95) for the same group in the pre-placement phase.
Conclusion: In this single UK NHS ambulance service study, we found a clinically important and statistically significant increase in appropriate non-conveyance rates by SPs who had completed a 10-week GP placement. This improvement persisted for the 12-month period following the placement and demonstrated cost savings compared to usual care.
导言:英国的NHS救护车服务非运输率约为30%,尽管非紧急病例有所增加,并且国家政策将紧急和紧急护理结合起来,为患者提供“正确的护理,在正确的地点,在正确的时间”。急诊科过度拥挤是病人面临的一个重大问题,导致护理质量下降,医疗费用增加,并可能增加死亡率。它还有助于增加救护车周转时间。约克郡救护车服务NHS信托(YAS)引入了一个专业护理人员(SP),以改善低急性病例的管理,但在这一组的非运输率没有预期的那么高。2018年,英国健康教育资助了一项试点计划,将护理人员轮岗到一系列医疗机构,在YAS, 10名护理人员在全科医生诊所实习了10周。本研究旨在评估初级保健安置是否以经济有效的方式适当地增加了SPs在10周全科医生安置后做出的不转移决定的水平和趋势。方法:我们使用2017年6月1日至2019年12月31日期间的事件数据进行了受控中断时间序列分析,以研究全科医生安置前后适当的非转移率。还进行了成本分析,检查了接受干预组SPs在安置前和安置后护理的患者每次适当的非运输的平均成本。结果:共有7349例由干预组SPs参与的事件符合纳入条件。在删除丢失数据的病例后,还剩下5537例(75.3%)。安置后,干预组与对照组相比,适当不转移率增加了35.0% (95% CI 23.8%-46.2%),适当不转移率下降了-1.2% (95% CI -2.8%-0.5%)。安置后,干预组sp的每个适当的非运输成本平均为509.41英镑(95%自举CI为454.92英镑- 564.26英镑),而同一组在安置前阶段的成本为1257.81英镑(95%自举CI为1233.42英镑- 1283.95英镑)。结论:在这项英国NHS救护车服务研究中,我们发现完成了10周全科医生安置的SPs的适当不分娩率在临床上具有重要意义和统计学意义。这种改善持续了12个月,与常规护理相比节省了成本。


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
