{"title":"The Utility of Transvaginal Ultrasound After Intrauterine Pregnancy Identification on Transabdominal Ultrasound in Emergency Department Patients.","authors":"Christopher Thom, Matthew Kongkatong, James Moak","doi":"10.2147/OAEM.S409920","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Ultrasonography has an important role in the evaluation of Emergency Department (ED) patients presenting with early pregnancy complaints. Both transabdominal (TAUS) and transvaginal ultrasound (TVUS) can be utilized. While TVUS generally allows for greater detail, it is unclear how much added benefit exists in performing TVUS once an intrauterine pregnancy (IUP) has been identified on TAUS.</p><p><strong>Methods: </strong>This was a retrospective study utilizing Radiology Department ultrasound examinations obtained in first trimester pregnancy ED patients during a consecutive four month period in 2019. Studies wherein both TAUS and TVUS were both performed were included. Two ED physicians with specialized training in point of care ultrasound reviewed only the TAUS images from these studies. Their findings were compared to the Radiologist interpretation, which was inclusive of both TAUS and TVUS components of the study.</p><p><strong>Results: </strong>108 studies met inclusion criteria. Amongst these, 82 had IUP's identified on the radiologist report. 69 studies had an IUP identified by ED physician review of the TAUS images, with 1 false positive. Each case of intrauterine fetal demise (IUFD) was identified on ED physician review of TAUS. Two ectopic pregnancies were present, neither of which was mistaken for IUP on ED physician TAUS review. There were 15 studies with subchorionic hemorrhage and 3 studies with an ovarian cyst noted on the radiologist report.</p><p><strong>Conclusion: </strong>Following the identification of an IUP on TAUS, the added diagnostic value of TVUS amongst this cohort of ED patients was low. Given the added time and cost of TVUS, selective instead of routine usage should be encouraged.</p>","PeriodicalId":74347,"journal":{"name":"","volume":"15 ","pages":"207-216"},"PeriodicalIF":0.0,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/bd/ab/oaem-15-207.PMC10237201.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/OAEM.S409920","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Ultrasonography has an important role in the evaluation of Emergency Department (ED) patients presenting with early pregnancy complaints. Both transabdominal (TAUS) and transvaginal ultrasound (TVUS) can be utilized. While TVUS generally allows for greater detail, it is unclear how much added benefit exists in performing TVUS once an intrauterine pregnancy (IUP) has been identified on TAUS.
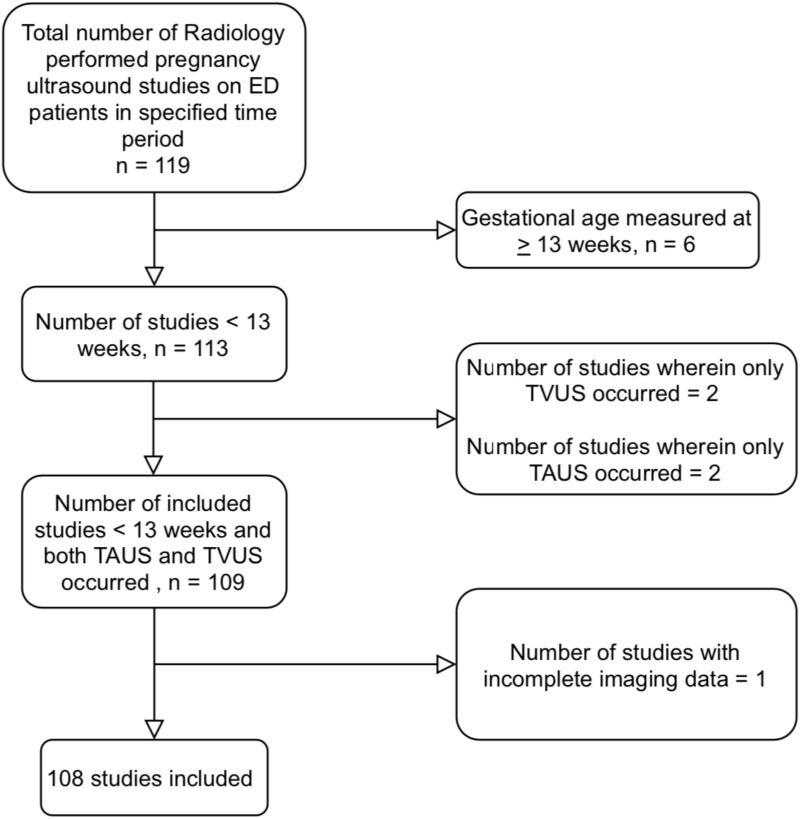
Methods: This was a retrospective study utilizing Radiology Department ultrasound examinations obtained in first trimester pregnancy ED patients during a consecutive four month period in 2019. Studies wherein both TAUS and TVUS were both performed were included. Two ED physicians with specialized training in point of care ultrasound reviewed only the TAUS images from these studies. Their findings were compared to the Radiologist interpretation, which was inclusive of both TAUS and TVUS components of the study.
Results: 108 studies met inclusion criteria. Amongst these, 82 had IUP's identified on the radiologist report. 69 studies had an IUP identified by ED physician review of the TAUS images, with 1 false positive. Each case of intrauterine fetal demise (IUFD) was identified on ED physician review of TAUS. Two ectopic pregnancies were present, neither of which was mistaken for IUP on ED physician TAUS review. There were 15 studies with subchorionic hemorrhage and 3 studies with an ovarian cyst noted on the radiologist report.
Conclusion: Following the identification of an IUP on TAUS, the added diagnostic value of TVUS amongst this cohort of ED patients was low. Given the added time and cost of TVUS, selective instead of routine usage should be encouraged.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
