Tae-Han Lee, Seunghun Lee, Bon San Koo, Kyung Bin Joo, Tae-Hwan Kim
{"title":"Radiographic involvement of cervical facet joints in ankylosing spondylitis: a longitudinal analysis in correlation with vertebral body lesions.","authors":"Tae-Han Lee, Seunghun Lee, Bon San Koo, Kyung Bin Joo, Tae-Hwan Kim","doi":"10.1186/s41927-023-00334-x","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The inability to assess structural changes in facet joints is a limitation of established radiographic scoring systems for ankylosing spondylitis (AS). We compared radiographic evidence of ankylosis in cervical facet joints and cervical vertebral bodies in patients with AS.</p><p><strong>Methods: </strong>We analysed longitudinal data collected from 1106 AS patients and assessed 4984 spinal radiographs obtained up to 16 years of follow-up. Comparisons between cervical facet joints and cervical vertebral bodies focused on the presence of ankylosis, which was defined by at least one facet joint exhibiting complete ankylosis (according to the method of de Vlam) or at least one vertebral body with a bridging syndesmophyte (according to the modified Stoke Ankylosing Spondylitis Spinal Score [mSASSS]). Ankylosis was assessed over time using spinal radiographs collected during follow-up periods stratified in 4-year increments.</p><p><strong>Results: </strong>Patients with cervical facet joint ankylosis had higher cervical mSASSS, sacroiliitis grades, and inflammatory markers, with more prevalent hip involvement and uveitis. Overall, the numbers of spinal radiographs indicating ankylosis were comparable between cervical facet joints (17.8%) and cervical vertebral bodies (16.8%), and they usually presented together (13.5%). We observed similar proportions of radiographs with ankylosis only in cervical facet joints (4.3%) and cervical vertebral bodies (3.3%). As damage progressed, configurations with both cervical facet joint ankylosis and bridging syndesmophytes became more predominant with longer follow-up times, while configurations with cervical facet joint ankylosis only or bridging syndesmophytes only were less frequently observed.</p><p><strong>Conclusions: </strong>Evidence of cervical facet joint ankylosis appears as often as bridging syndesmophytes on routine AS spinal radiographs. Presence of cervical facet joint ankylosis should be considered because it may have a higher disease burden.</p>","PeriodicalId":9150,"journal":{"name":"BMC Rheumatology","volume":"7 1","pages":"11"},"PeriodicalIF":2.5000,"publicationDate":"2023-06-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10245667/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMC Rheumatology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s41927-023-00334-x","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"RHEUMATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The inability to assess structural changes in facet joints is a limitation of established radiographic scoring systems for ankylosing spondylitis (AS). We compared radiographic evidence of ankylosis in cervical facet joints and cervical vertebral bodies in patients with AS.
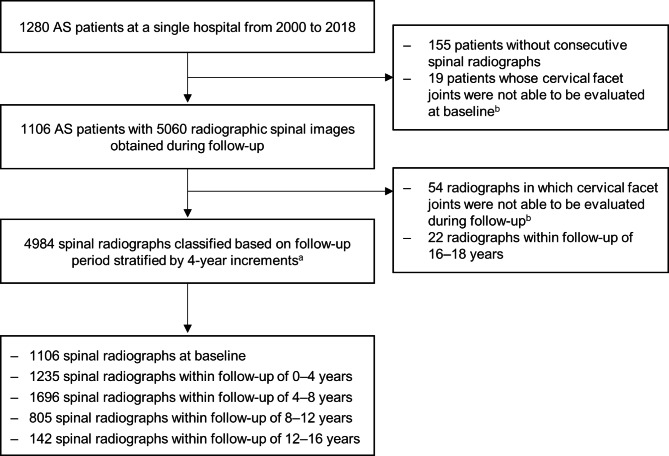
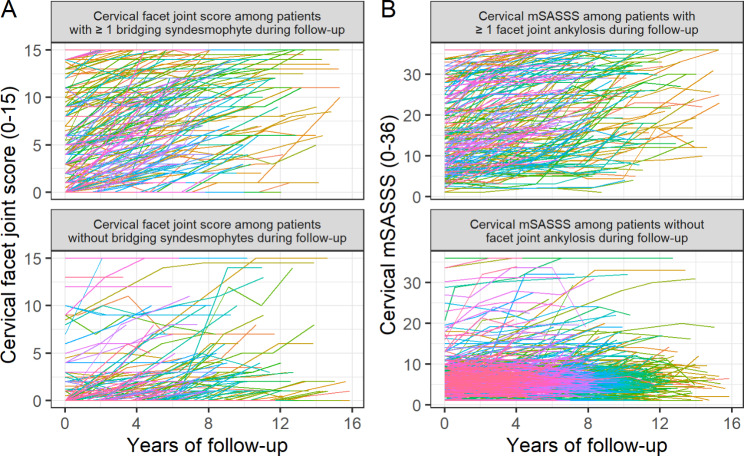
Methods: We analysed longitudinal data collected from 1106 AS patients and assessed 4984 spinal radiographs obtained up to 16 years of follow-up. Comparisons between cervical facet joints and cervical vertebral bodies focused on the presence of ankylosis, which was defined by at least one facet joint exhibiting complete ankylosis (according to the method of de Vlam) or at least one vertebral body with a bridging syndesmophyte (according to the modified Stoke Ankylosing Spondylitis Spinal Score [mSASSS]). Ankylosis was assessed over time using spinal radiographs collected during follow-up periods stratified in 4-year increments.
Results: Patients with cervical facet joint ankylosis had higher cervical mSASSS, sacroiliitis grades, and inflammatory markers, with more prevalent hip involvement and uveitis. Overall, the numbers of spinal radiographs indicating ankylosis were comparable between cervical facet joints (17.8%) and cervical vertebral bodies (16.8%), and they usually presented together (13.5%). We observed similar proportions of radiographs with ankylosis only in cervical facet joints (4.3%) and cervical vertebral bodies (3.3%). As damage progressed, configurations with both cervical facet joint ankylosis and bridging syndesmophytes became more predominant with longer follow-up times, while configurations with cervical facet joint ankylosis only or bridging syndesmophytes only were less frequently observed.
Conclusions: Evidence of cervical facet joint ankylosis appears as often as bridging syndesmophytes on routine AS spinal radiographs. Presence of cervical facet joint ankylosis should be considered because it may have a higher disease burden.
背景:强直性脊柱炎(AS)既有的放射学评分系统无法评估面关节的结构变化,这是一个局限性。我们比较了强直性脊柱炎患者颈椎面关节和颈椎体强直的影像学证据:我们分析了从1106名强直性脊柱炎患者中收集的纵向数据,并对随访16年的4984张脊柱X光片进行了评估。颈椎面关节和颈椎体之间的比较主要集中在是否存在强直,强直的定义是至少有一个面关节表现出完全强直(根据 de Vlam 的方法)或至少有一个椎体出现桥接联合骨赘(根据修改后的斯托克强直性脊柱炎脊柱评分[mSASSS])。随访期间收集的脊柱X光片对强直情况进行评估,每4年为一个阶段:结果:颈椎切面关节强直的患者颈椎 mSASSS、骶髂关节炎等级和炎症标志物较高,髋关节受累和葡萄膜炎的发病率较高。总体而言,颈椎面关节(17.8%)和颈椎椎体(16.8%)的脊柱X光片显示强直的数量相当,而且它们通常同时出现(13.5%)。我们观察到,仅在颈椎面关节(4.3%)和颈椎体(3.3%)出现强直的 X 光片比例相似。随着损伤的进展,随访时间越长,同时伴有颈椎面关节强直和桥状联合韧带增生的病例越多,而仅伴有颈椎面关节强直或桥状联合韧带增生的病例较少:结论:在AS脊柱常规X光片上,颈椎面关节强直的证据与桥状联合骨赘一样常见。颈椎面关节强直可能会造成更大的疾病负担,因此应予以重视。




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
